This series hopes to explore the history of British Antivaccinationism and Vaccine Scepticism. It is divided into 7 main eras: the period of Inoculation, 1721-1798; the introduction of vaccination, 1798-1853; the imposition of mandates, 1853-1898; the remaining history of the National Antivaccination League, 1898-1972; DTP Vaccine Scepticism 1972-1998; Andrew Wakefield and vaccines cause autism, 1998-2019, and Covid 19, 2020 to present. This section will look at the resistance from ordinary people to vaccination during the late 19th century.
Working Class Antivaccinationism
It had long been pointed out by antivaccinationists that the 1853 mandate was a piece of class legislation. Fines associated with non vaccination were easily payable by wealthy vaccine resistors, but ordinary resistors faced distraint (forced selling of their property) or prison.
Working class antivaccinationists saw vaccination as an attack and a threat to their bodies. They feared a threat to their employment (mandatory vaccination for employment), due to individual cases of employers attempting to force vaccination on their staff, particularly during an outbreak.
Working class people saw vaccination as an assault on their families. During the late nineteenth and early twentieth century, there was a belief among the elite that working class parenting, particularly working class mothering, was inadequate. Working class women were demonised for working (even though economic survival of the family depended on their income) and were seen as failing to contribute good children to a strong British race (see Anna Davin’s Imperialism and Motherhood). Working class people also perceived vaccination as a means of portraying their children as inherently diseased, and thus demonising them as the problem.
Vaccination was also linked to the New Poor Law, which compelled people into the workhouse if they were unable to find sufficient work to survive. The 1840 act which provided free vaccination was done via the Poor Law. Staff who were working in the vaccination program also worked in Poor Law administration. This associated vaccination with pauperism, a connection resented by working class people.
Resistance was associated with the East End of London, as well as certain working class towns, such as Leicester and Gloucester. It was also linked to other working class self improvement movements, such as the temperance movement. Examples of non compliance, other than the obvious refusing to vaccinate, included treating distraint sales as a protest venue, and physical assault against vaccination officers. (For more information about working class antivaccinationism, see the article ‘They Might as Well Brand Us’ by Nadja Durbach).
The largest display of resistance would occur in Leicester in 1885.
The Leicester Protest
Leicester was a hub of vaccination resistance. Antivaccinationist J. T. Biggs gives a very long account of Leicester and how the quarantine methods they employed after the 1871 smallpox outbreak were more successful than vaccination. Most of the city lost faith in vaccination after 1871, and there was a large amount of non-compliance with the vaccination edicts.
In 1885, there was a large protest against the mandatory vaccination laws in Leicester. This protest advocated for individual liberty and rejected the state control of working class children. Mothers stated that they wanted to protect their children from vaccination. The procession down the streets of Leicester included a horse and cow as the representations of vaccine lymph, furniture (as a representation of the distraint sales mentioned above) and an effigy of Edward Jenner. Further meetings also took place after the protest, stating the continued intent to resist vaccination.
Conclusion
Today, antivaccinationism is often portrayed by vaccinationists as a ‘privileged’ position advocated for by primarily middle-class mothers. If we look at history we can see this is far from the case and that many ordinary people were committed antivacciantionists.
This series hopes to explore the history of British Antivaccinationism and Vaccine Scepticism. It is divided into 7 main eras: the period of Inoculation, 1721-1798; the introduction of vaccination, 1798-1853; the imposition of mandates, 1853-1898; the remaining history of the National Antivaccination League, 1898-1972; DTP Vaccine Scepticism 1972-1998; Andrew Wakefield and vaccines cause autism, 1998-2019, and Covid 19, 2020 to present. This section forms part 3.2 looking at three main antivaccinationists active in the late nineteenth century, William White, Charles Creighton, and Edgar Crookshank.
William White
White authored a book called Story of a Great Delusion in 1885, looking at the history of inoculation and vaccination from an antivaccinationist perspective. It covers the entire period from the introduction of inoculation up to what was then the present day.
The book is primarily a historical account and he goes into detail not just about Jenner but the research of other important vaccinationists, such as George Pearson, another notable doctor, and William Woodville, doctor at the Smallpox Hospital in London. It explores their tense relationships and goes into more detail about Jenner’s personality (he had a significant habit of falling out with those who mostly agreed with him).
He also goes into the history of the government role in vaccination, such as the provision of vaccine lymph by the National Vaccine Establishment, and how £3,000 was budgeted for lymph, as an attempt to spread vaccination among the poor. He argues that Jenner’s ability to argue with everyone was one factor why government intervention was necessary to ensure the continuation of vaccination, rather than a reliance on private institutions.
He covers the introduction of the vaccine mandate – essentially the increasing intertwining between vaccination and government – and the introduction of ideological vaccine resistance, such as the founding of The Anti Vaccinator pamphlet by John Pickering.
Throughout the book he does make some arguments explaining why vaccination is a flawed practice, such as that it simply exchanges one disease for another while not decreasing death rate and that vaccine compulsion is purely about medical industry profit, rather than effectiveness. White believed the ineffectiveness of vaccination had been well demonstrated by the mandate introduction in 1853.
Charles Creighton
Dr. Creighton was a physician of note in the late nineteenth century, who completed a famous work on the history of epidemics in Britain. He was primarily interested in medical history rather than being a practicing doctor.
The story of how Dr. Creighton became an antivaccinationist is rather interesting. He was approached by the Encyclopedia Britannica to write an article on ‘Vaccination’ for their new edition. Feeling it was only justified to research the topic if he was going to write about it, he did – and became an ardent antivaccinationist. Perhaps surprisingly, the Encyclopedia agreed to publish whatever he wrote, so that edition ended up containing an antivaccinationist account.
He wrote two books condemning vaccination in 1887 and 1889.
His book Cowpox and Vaccinal Syphilis goes into great detail on the topic of vaccine lymph. This included the historical disputes between Jenner and Woodville, and whether the two sources were equivalent. Jenner had issues obtaining cowpox lymph for vaccination, and this whole issue tied into the debate about ‘spurious cowpox’, which was one of Jenner’s excuses for vaccination failure. The primary argument in the book in terms of the dangers of vaccination is that cowpox is completely unlike smallpox, and is actually closer to syphilis (which was historically known also as ‘great pox’). There had been an increasing number of deaths from infantile syphilis after the vaccine mandate was introduced. In Creighton’s view, cowpox was causing this syphilis increase.
Jenner and Vaccination is a more general work on vaccination as a whole. He argues that Jenner used sleight of hand to redefine cowpox as variolae vaccinae (which literally means, cow smallpox). This manipulation led people to accept similarities between the two diseases that did not exist. Jenner also defined cowpox as a mild disease despite significant issues of ulceration to gain support for vaccination. He also argues that because Jenner used a very mild form of inoculation (deliberate infection with smallpox) to ‘test’ whether or not the vaccinated had immunity, this led to false claims of immunity. The mild (known as Suttonian, after Daniel Sutton) method of inoculation caused only a small effect anyway, so it having little to no effect after a cowpox inoculation proved nothing. He also mentioned the redefinition of smallpox as chickenpox after vaccination to avoid accusations of vaccine failure.
Creighton became involved in the National Anti-Vaccination League, and ended up being excluded from the mainstream medical community.
Edgar Crookshank
Crookshank published two volumes addressing vaccination in 1889. The second volume is a compilation of essays about vaccination and varying vaccination experiments performed by its advocates. As such we will focus on the first volume as that contains Crookshank’s actual arguments.
History and Pathology of Vaccination makes several arguments. One of the most interesting is Crookshank’s analysis of Jenner’s two different versions of his original paper on vaccination. Jenner originally tried to publish a paper on vaccination in 1796 via the Royal Society, but they rejected the paper. Instead, Jenner published the paper himself in 1798. There are significant differences between the two. Jenner did add more experiments and cases in an attempt to bolster his argument (the original paper had only contained the vaccination of James Phipps, one case). He also sought to tone down the negative effects of cowpox in the new paper, and attribute issues with the disease as incidental effects not directly caused by cowpox/vaccination.
A second argument made by Crookshank is to discuss all the different sources that were used as vaccine lymph, explored further in this post.
Conclusion
This period was the height of Britain’s history of resistance to vaccines, and this included the number and intelligence of those resisting vaccination. There are many critics who I have not covered, also active during this time, such as William Tebb and Alfred Russel Wallace. But there was more than intellectual resistance – there was popular resistance from the working class, the topic of the next article in this series.
This series hopes to explore the history of British Antivaccinationism and Vaccine Scepticism. It is divided into 7 main eras: the period of Inoculation, 1721-1798; the introduction of vaccination, 1798-1853; the imposition of mandates, 1853-1902; the remaining history of the National Antivaccination League, 1902-1972; DTP Vaccine Scepticism 1972-1998; Andrew Wakefield and vaccines cause autism, 1998-2019, and Covid 19, 2020 to present. Because most active resistance to vaccination is clustered in this period between 1853 and 1902, Part 3 will have three sub-parts, discussing initial intellectual resistance in John Gibbs and Charles Pearce, the later intellectual resistance of William White, Charles Creighton, and Edgar Crookshank, and popular class resistance.
The Vaccine Mandate
In 1853, the United Kingdom introduced mandatory smallpox vaccination. There was a fine of 20 shillings introduced for non compliance. William White covers the introduction of this mandate in detail in his 1885 book, Story of a Great Delusion. According to White, the mandate was introduced because of the organised interests of the medical profession. There was a lack of discussion on the bill in Parliament, and White states it was an “act for application to the vulgar”, i.e. the working classes. In 1861 and 1867, the level of compulsion was increased, the 1867 amendments made non vaccination a continuous offense and gave the state the power to impose multiple fines.
Prior to the mandate, there was no organised antivaccinationism. There was personal distrust of vaccination among people, particularly the working class, and an apathy of not pursuing vaccination. The mandate triggered new wave of intellectual antivaccinationism, as well as popular vaccination resistance.
John Gibbs
John Gibbs was one of the first to write pamphlets against the vaccine mandate. In 1855 he wrote a letter opposing the mandate. He argued that the mandate was an attack on liberty, and that legislators freely admitted their ignorance on vaccination – relying only on the opinions of the medical profession to pass the bill. He argued that there were statistical issues with the case for vaccination, as there was evidence that smallpox was simply replaced by other causes of death and that there was no decline in the death rate due to vaccination. He also pointed to other diseases spread by vaccination, such as erysipelas (a form of skin rash and swelling), tuberculosis and syphilis.
He drew attention to the moral issues with government forcing a medical intervention on the people and that this opposed self responsibility. Vaccination was in his view “a state religion in physic”.
Charles Pearce
Charles Pearce was an editor of a medical journal, who received papers from Gibbs, and as a result became an antivaccinationist. In 1868, he authored the short book, Vaccination Its Tested Effects, arguing that “vaccination is a crime against nature”.
Pearce points to the theory behind vaccination, that is the idea that cowpox and smallpox are “governed by the same laws” as an error believed by Jenner. He argues that vaccination is not even practised according to Jenner’s theory, since Jenner believed in a chain from horse-cow-human. Vaccine lymph had been spread from human to human for many decades at this point, and had not been anywhere near passage via a cow. He also pointed to the introduction of revaccination as a contradiction to Jenner’s theory of life long protection from vaccination.
He argued that smallpox vaccination did not save lives, by arguing that smallpox increased longevity if you survived, by the fact that there was an increase in mortality from measles after compulsory vaccination was introduced, and that smallpox vaccination could spread syphilis. He points out that there were ups and downs in smallpox due to the laws of epidemics. He believed sanitation and hygiene were the best methods to combat smallpox mortality.
Conclusion
There was increased intellectual resistance to vaccination after the smallpox vaccine mandate was introduced. This would continue to develop further, and British antivaccinationism would reach its peak between 1880-1902 with the cases made by William White, Charles Creighton and Edgar Crookshank against the practise.
Polio vaccines are hailed as a heroic development in medicine and science. However, there is a dark side that is less acknowledged, at least in the media accounts of the polio vaccine. This is the abuse of disabled people – specifically disabled children in institutions – by vaccine testers.
How the Sausage was Made
Most polio vaccine development took place using monkeys. Jonas Salk, who created the inactivated polio vaccines, used rhesus monkeys imported from India extensively. In fact, this import of monkeys was a minor industry. This testing had involved infecting multiple monkeys with the virus, particularly when Salk had been involved in attempting to discover the amount of different strains of poliovirus. It also involved extraction of the monkey kidney tissue, in order to create a cell culture to grow the virus to create the vaccine. It was required to keep killing monkeys to gather this tissue because immortal cell lines, such as the HeLa line (an immoral exercise in lack of informed consent and medical racism in itself) had not yet been created when the polio vaccine was being developed. This cell line would only come to be used in a limited way during the testing phase.
However, Salk and other vaccine testers needed to move their vaccine testing from primates to humans, before the full scale testing that would take place among the general child population. For this exercise, they selected children in institutions as the first target for human vaccine testing. As quoted in the article Between Simians and Cell Lines:
The transition from experiments with imported non-human primates to trials with ‘normal’ American children was conceptually bridged via the testing of institutionalised disabled humans deemed non-normal.
Let’s take a closer look at the three main vaccine developers at this time, Jonas Salk, Albert Sabin, and Hilary Koprowski, and how they used disabled children in their vaccine experiments.
Jonas Salk
Jonas Salk, while testing his inactivated polio vaccine, carried out two rounds of testing on disabled children. He carried out work at the D T Watson Home for Crippled Children and the Polk State School. This testing took place in 1952, prior to the main testing of the Salk vaccine in 1954:
At Polk, Salk first inoculated children who were already polio victims with a vaccine derived from the same virus type present in their blood to assess their immune response. Following this, he vaccinated other children who had not previously contracted polio and who lacked protective antibodies.
There is no even hypothetical benefit to these children if they had already had polio.
However Sabin’s application to test his vaccine there was refused, and he turned to prisoners to test his vaccine instead.
Hilary Koprowski
Hilary Koprowski is the least well-known of the three main polio vaccine developers in the 1950s. This is because his vaccine was not adopted. However, it was extensively used in some parts of Africa, particularly the then Belgian Congo around Leopoldville (modern Kinshasa).
Koprowski, like Sabin, believed only a live vaccine would be effective against polio. He thus worked on creating attenuated strains of the poliovirus.
In 1950, he gave the first live polio vaccine to a human being at Letchworth – a home for people with intellectual disabilities. In the articles published about the vaccine testing, the children given the vaccine were referred to as ‘volunteers’. One of these children had to be fed the vaccine via a stomach tube.
While working on further attenuated viral strains, he created his most notable polio vaccine strain, known as CHAT. He created this vaccine strain by attenuation the virus in various cell lines. However, he then used the disabled children at Sonoma institution to create the vaccine strain itself, by passing the attenuated vaccine strain via four children and extracting the virus from fecal matter. He called the vaccine CHAT, according to him, because it was a truncation of Charleton, who was the last child used in the creation of the strain.
He conducted further trials at Sonoma in 1955, including those to see whether his attenuated vaccine strains would spread to non- vaccinees. As stated on page 221 of Edward Hooper’s book, The River:
In the course of these he and Tom Norton, assisted by a phalanx of nurses, had conducted two contact experiments, in one of which a group of six children who had been fed SM [one of Koprowski’s strains] and who were excreting virus in their stools were kept “in very intimate contact” with another eight children who lacked Type 1 antibodies. In practice, this meant that for the next twenty days the children (all of whom were incontinent) were allowed to play together for three hours a day on a plastic mat, which, although it was washed down to prevent its becoming grossly soiled, was deliberately not disinfected. In the course of the experiment, three of the unvaccinated children became infected with Type 1 virus.
Conclusion
Disabled children in institutions were an easy and convenient source of ‘raw material’ for vaccine testers. All three polio vaccine ‘pioneers’ tried to test their vaccines at disabled institutions and two actually did so.
Back in February 2023, I wrote about a case from Jersey, where a severely autistic man injured by the MMR vaccine was being forced to take the Covid vaccine against the will of his parents. He was too severely autistic to make his own decision regarding the vaccine. The care home where he was living had denied him certain activities and essentially kept him in isolation from the other residents because he was not vaccinated.
Amother has launched a legal battle to stop the state from spiking her Down’s syndrome son’s drinks with sedatives so he can be jabbed with the Covid vaccine, The Telegraph can reveal.
Cups of tea and glasses of orange juice have been secretly laced with sedatives to subdue the man, in his thirties, so he can be given the vaccine and booster jabs.
I don’t have words for how utterly disgusting and repulsive this is. The people doing this are either psychopaths, or so sick in the head off the high of vaccinationism that they cannot even comprehend moral values any more.
Despite all the side effects of the covid vaccine, they are still pushing the ‘benefits outweigh the risks’ narrative as a justification to push the vaccine.
Here is a description of how the forced sedation was carried out from the above article.
As a “thank you” for having a mug of breakfast tea and a glass of orange juice brought into his room, Adam invariably hugged the staff he trusts so implicitly at his care home.
Unbeknown to him, on five separate occasions over the last 16 months those drinks were laced with a “covert anxiolytic medication” – a powerful sedative. Twice he became groggy before eventually succumbing to a deep sleep.
Each time, a team of senior carers, a nurse and the home’s manager stood quietly outside the room awaiting the nod to enter. One of them was armed with a syringe – kept well hidden due to Adam’s needle phobia – loaded with the Covid vaccine.
When the sedatives worked, Adam’s sleeve was quickly rolled up, the antiseptic wipe swiped over his upper arm and the needle inserted deep into his muscle as the plunger was pressed emptying the syringe barrel of its viscous contents. One carer made copious notes in readiness for a report which would be sent to the Court of Protection explaining how the procedure had gone.
The article further states that when Adam was given information relating to the vaccine, he said no to the vaccine.
Since the 1990s, the idea of ‘neurodiversity’ has become a cottage industry. The basic tenet of neurodiversity is that autism is a perfectly normal variation of human development that should not be seen as a negative trait. It seeks to highlight the alleged ‘positive’ traits of autism and believes that the struggles of people with autism are largely caused by society not being accepting rather than the inherent downsides of the condition. This article will seek to discuss three parts of this phenomenon by comparing two theories of autism: the neurodiversity theory of autism and the iatrogenic theory of autism i.e. vaccine injury. The first part will discuss the evidence for each theory, concluding that vaccine injury has a large amount of evidence to support it. The second part of this article will look at the individuals and institutions that promote each theory and how the media portrays each group. The third part will draw it together by explaining how the neurodiversity theory is constructed as an alternative to deflect from the vaccine injury theory and to gaslight people suffering with autistic vaccine-injury and their parents about their experiences.
Part I: Two Theories
There are two main theories of autism. The first theory states that autism is genetic, and the second theory states that autism is iatrogenic. The first theory is advocated by both people who think that autism is a good thing, and by those who think it is a bad thing. The latter group of people, who believe that autism is a net negative but who also believe it is genetic, will not be discussed in this article. Instead we will be comparing the ‘autism is a positive, genetic gift’ group (the ‘neurodiversity’ group) to the ‘autism is iatrogenic, largely caused by vaccination’ group (the ‘vaccine-injury theory’ group). Part I will outline these two theories and look at the evidence.
The Neurodiversity Theory of Autism
What is the ‘neurodiversity’ theory of autism? It can be summed up by saying that autism is not a disability, it is a difference that should be celebrated. If you search for ‘neurodiversity’ you can find all sorts of articles advocating for this. Here’s one picked at random:
Neurodiversity is a movement that wants to change the way we think about autism. It rejects the idea that autism is a disorder and sees it instead as a neurological difference: one with a unique way of thinking and experiencing the world.
The movement focuses on celebrating neurological diversity and championing the different world-views and skills that autistic, dyslexic, bipolar, and other neurodiverse people have.
The idea of ‘neurodiversity’ has been increasing in popularity as a paradigm to ‘explain’ autism.
Of course, saying that autism is a positive trait does not explain it. So neurodiversity theorists use genetics to explain autism.
I will argue that both sides of the neurodiversity coin are false: having autism is always a negative thing, and that genetics does not explain autism.
Let’s start with the genetics aspect. One significant piece of evidence that the autism-is-genetic advocates use is twin studies:
Since the first autism twin study in 1977, several teams have compared autism rates in twins and shown that autism is highly heritable. When one identical twin has autism, there is about an 80 percent chance that the other twin has it too. The corresponding rate for fraternal twins is around 40 percent.
On the surface, twin studies look like exceedingly convincing evidence. They have been used to argue for a genetic link for a varying range of problems, including schizophrenia. In reality, though, twin studies are not good evidence that autism is genetic.
The problem that we run into is that twins are likely to have had the same environmental exposure, and this is doubly true when it comes to vaccination. No parent is going to vaccinate one of their twins and not vaccinate the other in some sort of science experiment. Thus both twins will be getting very similar exposure to aluminium, thimerosal, etc. via vaccinations. (Though see this caveat: aluminium levels in vaccination can vary significantly when vials are actually examined). The other major issue with twin studies is that they conclude that interaction between the body and these kinds of exposures is ‘genetic’. A genetic propensity to, say, accumulate certain toxins may well exist in autism cases. But in order for autism to develop, exposure to the toxin is required, and exposure to a toxin is not genetic. The same weakness applies when looking at alleged genes that have been associated with autism – it could be that those genes simply predispose a person to toxin accumulation.
The main weakness in the genetic case for autism is below:
It goes without saying that human genes have not radically changed since 1970. So how can the autism rates have changed so drastically? Autism-is-genetic advocates have tried their best to explain this graph, but they have done a bad job of it, because the whole graph screams ‘environmental causes’. But let’s have a look at their explanations for an increase in autism.
The main explanation offered is that the definition of autism has got wider and that is why these numbers have increased so much. Intuitively, this is a really poor explanation, for a number of reasons. For a start, we are looking a massive, massive increase. 1 in 10,000 to 1 in 30 is huge. To explain this simply by stating ‘it’s increased diagnosis’ is intuitively and logically implausible. People who argue this, I think, don’t understand how large a proportion of the population 3% is. That is a very significant chunk of the population. Older people here can employ their common sense. Were 3% or more of your childhood colleagues autistic? If you doubt that you could tell, I assure you that you can with just a little thought. Poor eye contact is a dead giveaway for autism, as is just an obvious awkwardness. The reality is, even ‘high functioning’ autistic people just seem odd, weird and off in particular ways so I would say you could almost always tell. Furthermore, the unemployment rate for people with autism, according to UK government data, is 78%. If we approximate the data, if 1 in 30 people are autistic and 2/3 (being generous) cannot work, this means around 2% of the population cannot work due to autism. The idea that government institutions never noticed 2% of the population being unemployable due to autism is laughably implausible.
This hypothesis also does not fit the shape of the graph very well. It keeps curving upwards, rather than seeing a bump for a change in diagnostic criteria and a levelling. The graph has still not levelled off. At some point, you have to start asking questions.
This issue also becomes more difficult to cover up when you consider severe autism. Autistic people who have a basic level of functioning in the ‘real world’ may just come across to normal people as a bit weird. In these people’s case, it’s more possible that they may not have a diagnosis. This would not be the case with those with severe autistic deficits. Again this is another argument that is just absurd on the face of it:
You can’t have missed 97 percent of the children in the ’80s who had autism. They’re trying to get the public to believe that kids who spin in circles, don’t speak, don’t socialize, can’t go to the bathroom by themselves all existed in our public high schools and elementary schools in the ’80s but only today have gotten a proper diagnosis. It’s incomprehensible.
Aside from being intuitively implausible, one study on this issue concluded:
In summary, the incidence of autism rose 7- to 8-fold in California from the early 1990s through the present. Quantitative analysis of the changes in diagnostic criteria, the inclusion of milder cases, and an earlier age at diagnosis during this period suggests that these factors probably contribute 2.2-, 1.56-, and 1.24-fold increases in autism, respectively, and hence cannot fully explain the magnitude of the rise in autism.
But what about the claim that autism is always a net negative? Surely that’s a little bit fundamentalist? After all, some of the advocates of the neurodiversity theory are autistic themselves, right, and surely they would know? So let’s tackle this thorny question.
The most obvious piece of evidence to start with is life expectancy. The evidence demonstrates that autism significantly decreases life expectancy. This is pretty mainstream evidence that can be found with a quick search.
One study, published in the American Journal of Public Health in April 2017, finds the life expectancy in the United States of those with ASD to be 36 years old as compared to 72 years old for the general population.
In other words, according to this study autism halves life expectancy.
The other study was published by the British Journal of Psychiatry in January 2018. This was a Swedish study showing similar results but elaborating on other causes of death as well. This study showed a life expectancy in those with ASD with a cognitive disability (or a learning disability) at 39.5 years versus 70 years for the general population studied. Those with ASD without a learning disability had an average age of death at about 58 years.
Furthermore, most of these causes of death are inherent to autism. For example, being much more likely to die in an accident. Autistic people have poor motor control and are much more likely to have these kinds of accidents such as drowning that lead to death. Horrific anxiety at normal experiences, such as sensory issues around normal noise/light/smell stimuli, also increases mortality as the body becomes overwhelmed with the constant anxiety triggers, meaning that the body’s ability to fight cancers is impaired, and heart attack and stroke risk is increased. People with autism are also unemployed/unemployable, with only about 20% of autistic people even being employed in the UK. This is linked to having awful social skills, having severe anxiety, and in some cases being completely non verbal and non functional. Being perennially unemployable is bad for your health; higher unemployment rates have been well established to be linked to mortality in sociology.
A study that followed autistic people for 20 years showed even more negative outcomes, although most of the participants also had other intellectual disabilities.
The outcome data was grim, showing pervasive inability to live independently, hold a job, or manage money. Few became independent, with 99% unable to live independently. Of those, 70% lived at home with relatives, 21% lived in disability homes in the community, and 8% in residential facilities. A mere 3.7% attained postsecondary education, about half of those representing certificates from college disability programs. While the majority were considered incapable of holding a job in the competitive workspace, some worked in disability workshops or other sheltered positions. Most participants were incapable of handling money, even with caretaker assistance, with only 9.5% considered capable.
The neurodiversity paradigm likes to attempt to escape from this reality by claiming that this is purely down to ‘society’ refusing to accept us. That argument is nonsense. The argument is most obviously flawed when it comes to those with severe autism, since any range of accommodations will not fix deficits such as being non verbal, not being able to go to the toilet by yourself, seizures (comorbid with autism), extremely poor motor control, severe gastroenterological issues (linked to autism), sensory issues and meltdowns, etc. If a neurodiversity advocate would like to explain how ‘acceptance’ will fix these problems, the comment section is all theirs. But it is even pretty much nonsense when it comes to ‘high functioning’ autism as well. The reality is ‘acceptance’ and accommodations only really make a difference in edge cases when it comes to solving the issues outlined above. Take for example ability to work. The severely impaired autistic person will never be able to work, you can throw all the accommodations in the world at the issue, it’s not going to happen. Whereas, a high functioning or borderline high functioning autistic person may be able to work if given a few accommodations. I’m not arguing against accommodations. What I am arguing against is the idea that accommodations, or society being more accepting of autism will fix our problems. It won’t.
As for the supposed ‘positive’ aspects of autism, what are they? Usually, it is claimed that many people with autism are more intelligent and analytical than normal people. However, this is likely to confuse correlation and causation. The most plausible explanation here is that brain development is more likely to be disrupted by toxins in the case of intelligent people due to more dense neuron growth in highly intelligent people. And again, severe cases of autism are erased by this view. It glorifies a very narrow spectrum of individuals with autistic injury – the ‘autistic savant’ – while writing off the harms done to the rest.
So what about the people with autism diagnoses who make the claim that autism is a positive thing and that neurodiversity is valid? Well, if someone with an autism diagnosis saying something settles the question, then autism is a devastating vaccine-injury that destroys and obscures the true personality of the individual, rather than reflecting it. Because of course this author has an autism diagnosis. So this kind of argument gets us nowhere.
The Vaccine-Injury Theory of Autism
There is an alternative, ‘underground’ theory of autism which advocates for the view that autism is (at least primarily) caused by vaccination. This article will discuss one cause of autism that the author believes has been comprehensively documented, that is aluminium adjuvants in vaccination entering the brain, disrupting the housekeeping cells of the brain (glia and microglia)and triggering inflammatory reactions such as the il-6 pathway. This is not to say that there are no other problems with vaccination as it relates to autism or no other possible causes (e.g. thimerosal). This article will stick to one cause for reasons of length and clarity.
I will go into a little bit more detail on the basic theory, before discussing the evidence. Aluminium is used in ~80% of vaccines as an adjuvant (substance used to promote an immune response). It is in the vast majority of childhood vaccines, excluding the MMR. However, aluminium is also a neurotoxin that the body cannot filter out effectively when injected, and because of this it can enter the brain. In short, the mechanism of how the injury occurs is like this. The aluminium in a vaccine is injected into the body. Immune cells are stimulated to respond to the site of injection. These immune cells (macrophages) respond and ‘swallow’ the aluminium. But when any inflammatory event in the brain occurs, these cells will be called upon to help, but instead will bring a massive payload of toxic aluminium with them into the brain.
A set of nine criteria used to determine the strength of an association between a disease and its supposed causative agent. They form the basis of modern medical and dental epidemiological research.
The more of the Bradford-Hill criteria you can demonstrate, the more likely it is that A causes B. Let’s look at these criteria with relevance to the fact that vaccines cause autism.
The first factor we can discuss is coherence. In other words, “does the association fit with other facts?” In the case of the above theory, it fits very well with facts about aluminium.
Aluminium is toxic to the human body. Aluminium has no biological function in human life and so its presence in the human body is always a net negative. The idea than aluminium, at least, can be toxic is widely accepted. Furthermore, it is accepted that aluminium can enter into brain tissue. Even more than this, it is accepted that it can cause harm once it gets into the brain tissue. One form of aluminium toxicity where this occurs has been observed in dialysis patients:
[A]luminium toxicity occurs due to contamination of dialysis solutions, and treatment of the patients with aluminium-containing phosphate binding gels. Aluminium has been shown to be the major contributor to the dialysis encephalopathy [“damage or disease that affects the brain”] syndrome and an osteomalacic component of dialysis osteodystrophy.
In stating this so far, I haven’t deviated from accepted science. Slightly more controversial than this is the idea that Alzheimer’s is caused by aluminium in the brain. This idea has been around since 1965 according to the Alzheimer’s Society. Although some people doubt the correlation-causation relationship (I would argue more for financial reasons than scientific), there is evidence from a wide range of sources.
The Scotsman reported on a study performed by researchers looking at aluminium levels in drinking water that found people in areas with higher levels of aluminium were more likely to die of dementia. The study’s author said:
We still see this well accepted finding that higher levels of aluminium in particular are associated with an increased risk of dementia. It’s confirmatory rather than anything else. [my emphasis]
Dr. Chris Exley has done multiple studies showing high levels of aluminium in the brains of those who died with a diagnosis of Alzheimer’s disease.
Animal studies also provide further evidence for the fact that aluminium in injurious to the brain. Dr. Christopher Exley observed, when he was studying fish, that when the fish were exposed to aluminium, they would start hanging out in the corner of the tank. Another study, performed by a sheep farmer (and shown in the Bert Ehgartner documentary, Under the Skin), showed that sheep injected with aluminium adjuvant (even without an antigen) showed much higher levels of aggressive behaviour and did things like grind their teeth on metal railings. Mice are also negatively affected by aluminium:
Male mice in the “high Al” group showed significant changes in light–dark box tests and in various measures of behaviour in an open field. Female mice showed significant changes in the light–dark box at both doses, but no significant changes in open field behaviours.
Thus, aluminium was clearly affecting the neurochemistry of the animals, and these behaviours are decent proxies for autistic symptoms in humans (aggression being analogous to autistic meltdowns and the fish acting strangely being analogous to social avoidance).
All of this evidence is a strong case that the aluminium factor in autism is coherent. We know aluminium is toxic and can harm the brain. Therefore that it can cause the kind of behavioural issues that we observe in autism cannot be prima facie ruled out. This is Criteria 1 on our Bradford Hill list solidly met.
The next criteria we can discuss is dose-response relationship. In short, if we give more aluminium adjuvants to children, do we see an increase in autism? Recall our graph from above – the 1-in-10000 to the 1-in-36 increase in autism prevalence. Now let’s compare this to the increase in aluminium adjuvants and thus exposure.
Shaw and Tomljenovic wrote a paper addressing this topic:
By applying Hill’s criteria for establishing causality between exposure and outcome we investigated whether exposure to Al from vaccines could be contributing to the rise in ASD prevalence in the Western world. Our results show that: (i) children from countries with the highest ASD prevalence appear to have the highest exposure to Al from vaccines; (ii) the increase in exposure to Al adjuvants significantly correlates with the increase in ASD prevalence in the United States observed over the last two decades (Pearson r=0.92, p<0.0001); and (iii) a significant correlation exists between the amounts of Al administered to preschool children and the current prevalence of ASD in seven Western countries, particularly at 3-4 months of age (Pearson r=0.89-0.94, p=0.0018-0.0248).
The correlation here is strong – more doses, more autism. The dose-response relationship is in this data. Point 2 on the Bradford Hill Criteria list is met.
The third factor that we can discuss is strength of association. Or in other words, how much is the difference in observed rates of autism between the vaccinated and the unvaccinated? This question is not all that easy to answer, mostly because information on this kind of question has been suppressed.
Dr. Paul Thomas has revealing evidence on this question.
Dr. Paul Thomas is the most successful doctor in the world at preventing autism. Data from his practice show:
If zero vaccines, autism rate = 1 in 715;
If alternative vaccine schedule, autism rate = 1 in 440;
If CDC vaccine schedule, autism rate = 1 in 36.
[…]His alternative vaccine schedule reduces autism risk by more than 1200%. However even an alternative vaccine schedule increases autism risk by 160% versus no vaccines at all.
The difference between 1 in 715 and 1 in 36 is huge. This is evidence of a significant strength of association between two factors. Of course the historical evidence showing fewer cases of autism among older people and more among the young with a strong correlation also matches up with this evidence, since older people are comparatively ‘unvaccinated’. So that’s our third criteria met.
The fourth factor we can discuss is temporal relationship. In other words, the effect must follow, not precede exposure. This factor is difficult to elucidate with vaccines, because exposure is so early on in life, including in the first day of life in the US. This is used by the vaccine cult to argue for the genetic position, but also ensures that it is more difficult to prove that exposure causes the symptoms because the exposure is so early and rampant. However, the simple observation of vaccines preceding autism is almost always true (unless the child is unvaccinated) because if you expose the child at day 1 (US) or 2 months (UK) that is before autistic behaviour is observed. So in a way, their rampant pushing of vaccinations has met this criteria all by itself.
We also haveanecdotal evidencefor this factor, that is, parents observing their child regressing into autism after vaccination. Of course, anecdotal evidence is automatically dismissed by any Pharma apologist. It is true that when using anecdotal evidence, there are significant pitfalls to consider. People can misremember things, or actively lie. These points are worthy of consideration.
However, both of these risks are minimised in the case of assessing autistic regression after vaccination. In terms of lying, there is simply no motive for a parent to lie about observation of regression into autism after a vaccine. Suggesting to a paediatrician, for example, that a child’s autism was caused by a vaccine will lead to being attacked and dismissed by the doctor. Parents are also attacked in the media if they suggest this idea, such as in the case of Jenny McCarthy, who has been subject to hit pieces because she stated that the MMR vaccine caused her son’s autism. Although vaccine advocates state that parents are likely to fall for the idea that someone is to blame for their child’s autism (such as doctors or Pharma) this is also unlikely. The parents had to consent for the vaccine to be given, and so you would expect to observe the opposite: parents denying that vaccines cause autism, since then they would have to blame themselves for consenting to the vaccine(s) and human beings do not like to acknowledge guilt.
Being mistaken about observation is also less likely in the case of autistic regression. This is because we are talking about parental observation of children and decent parents are highly alert to any signs of illness in a child, particularly a child of the age likely to receive vaccines. I will concede however that it is not impossible for someone to either be mistaken or lie. However it is quite implausible that given the factors weighing against these that all cases are examples of lying or misremembering given the multitude of testimonies that we have.
Thus there is at least some evidence for criteria four on the Bradford-Hill list.
The fifth factor that we can discuss is consistency. In other words, if we introduce aluminium adjuvants to all sorts of different groups, rich, poor, black, white, Asian, male, female, etc, do we see increased levels of autism?
There is a male-female disparity in autism diagnosis, with males being significantly more likely to be diagnosed than females. There is likely some biological reason why boys are more susceptible to this form of aluminium poisoning that is currently unknown (or at least, unknown to me). Nevertheless we see an increase in autism diagnosis in both groups.
The sixth factor we can discuss is experimental evidence. In other words, do we have any hard evidence for aluminium in the brain in autism? The answer to this is yes.
Dr. Exley and his research team examined this question directly. They obtained samples of brain tissue from individuals that had died with a diagnosis of autism. This was the first study of this kind. They examined this brain tissue and found very high levels of aluminium in all samples.
The aluminium content of brain tissue in autism was consistently high. The mean (standard deviation) aluminium content across all 5 individuals for each lobe were 3.82(5.42), 2.30(2.00), 2.79(4.05) and 3.82(5.17) μg/g dry wt. for the occipital, frontal, temporal and parietal lobes respectively. These are some of the highest values for aluminium in human brain tissue yet recorded and one has to question why, for example, the aluminium content of the occipital lobe of a 15 year old boy would be 8.74 (11.59) μg/g dry wt.?
We can add another one of Exley’s papers to make this evidence even better. This paper by Exley and Clarkson contains control samples who died with no signs of neurodegenerative disease:
The aluminium content of each lobe (mean and SD) were 1.03 (1.64), 1.02 (1.27), 0.95 (0.88), 0.77 (0.92) and 0.51 (0.51) μg/g dry wt.
These samples have much lower levels of aluminium in them than the autism samples, and this is despite the fact that the controls were mostly older than the autism samples – meaning lifelong exposure to aluminium through non-vaccine routes would have been higher and it would have had more time to accumulate in the control tissues.
The main limitation of this evidence as pointed out by its critics is that the study had a small sample size of N=5 when it came to measuring aluminium concentration in the autism samples (and for some aspects of the study N=10). This was for practical reasons (i.e. there isn’t a large amount of samples of autistic brain tissue available).
It is fair to acknowledge this, and obviously it would be better if the sample size was larger. However, it is completely dishonest to dismiss this study because of the small sample size. This study, for example, is completely different from a survey where 5 participants answering would be worthless. We are looking at pathological brains with clear evidence of a high level of a neurotoxin in them. The level of neurotoxin in these brains cannot be explained away by saying that there is only a few of them. To have that level of brain aluminium content and for it to not be pathological and negatively affecting the cells around it is absurd, unless you want to straight up deny that aluminium is neurotoxic.
Furthermore, no-one has tried to either confirm or reject the Aluminium Research Group’s findings (to this author’s knowledge at least). The establishment haven’t done a study where they demonstrate that the levels of aluminium found by the group are overly high. This is another case where the establishment claim the evidence isn’t good enough to support an anti-establishment view and then just ignore the question. So, despite establishment criticisms, this is criteria six on our Bradford-Hill list met.
We can use Exley’s evidence to discuss the seventh criteria, biological plausibility.
The 2018 paper shows that the high levels of aluminium were found associated with glia and microglia:
Discrete deposits of aluminium approximately 1 μm in diameter were clearly visible in both round and amoeboid glial cell bodies (e.g. Fig. 3b). Intracellular aluminium was identified in likely neurones and glia-like cells and often in the vicinity of or co-localised with lipofuscin (Fig. 5). Aluminium-selective fluorescence microscopy was successful in identifying aluminium in extracellular and intracellular locations in neurones and non-neuronal cells and across all brain tissues studied (Fig. 1, Fig. 2, Fig. 3, Fig. 4, Fig. 5).
This is important because those cells are disrupted in autism. For example, they are responsible for synaptic pruning, which does not occur correctly in autism.
Aluminium-loaded mononuclear white blood cells, probably lymphocytes, were identified in the meninges and possibly in the process of entering brain tissue from the lymphatic system (Fig. 1).
The eighth criteria we can discuss is specificity. The idea of specificity ideally means that one disease has one cause, but this is difficult to apply to reality as Bradford Hill acknowledged. Aluminium adjuvants, in reality, are highly likely to cause more than one disease. However, the argument is not just that aluminium adjuvants cause autism, but that a specific action of aluminium adjuvants causes autism. Our theory offers a specific toxicant (aluminium), a specific route of exposure (injection), a specific method by which that toxin gets into the brain (macrophages), specific cells that are disrupted (glia and microglia), and specific negative cascades that are triggered (excessive IL-6 production due to an inflammatory response). Our argument also does not claim that glial disruption by aluminium adjuvants causes a whole host of problems, but autism specifically (and nothing else). So the theory meets criteria eight on the list.
The last factor we can discuss is analogy. If we can observe similar things happening that makes our own theory more likely to be true. This is easy to demonstrate in the case of aluminium poisoning, as poisoning by different metals, such as mercury, can cause significant impairments in child functioning. One interesting case worthy of discussion here is that of acrodynia. Acrodynia, or ‘Pink disease’ was an early 20th century disease that symptomatically had some overlap with autism although with some differences. It was later proven that pink disease was a form of mercury poisoning caused by mercury teething powders. We know from this case that metal poisoning can cause symptoms with some similarities to autism. There are also examples of aluminium itself causing other forms of poisoning, which were discussed in point 1. So analogy also supports our case and gives us point 9.
Conclusion
As we can see from the above discussion, the idea that vaccines cause autism is strongly evidenced. However, the theory is also opposed by the entire establishment despite this evidence. It is to how these two differing theories of autism are treated that we now turn.
Vaccination was invented during the transition from the feudal age to the capitalist age, the transition from the spiritual age to the scientific age. As such vaccination is touted as one of the major achievements of that scientific age that is said to mark human progress. The official narrative regarding vaccination is this upward trajectory of saving lives through the conquest of disease. As Nature is subjected to conquest by the machines of the Industrial Revolution, and the ‘savages’ that represent Nature are subject to conquest by the gun, Nature’s ‘weapon’ against Man, disease, is subject to conquest by the needle.
Such a narrative, of course, is entirely reductionist: as the holistic skill of the artisan was reduced to excruciating specialism in a tiny part of a whole by the capitalist mode of production, the intricate complexity of the human immune system, with interlocking parts not fully understood by even the most advanced immunologist, is reduced to a crude production of antibodies by vaccination. The inevitable interplay of microbes and humans – distorted by the strain of industrial societies on the human immune system – is reduced to a one sided narrative of war.
Vaccination is the conquest of nature, but also represents the domination of man over woman, male supremacy. Before the modern era medicine was often the preserve of the wise woman or witch. The demonisation of such women was vital, crucial for the domination of the male doctor to fully emerge. Vaccination is merely the ultimate step in that domination. Forgive me a little psychoanalytic speculation – the injection is his hard, throbbing prick; through it the doctor spreads his seed and creates twisted, broken children in his image, this makes him a god. Mother speaks reality, ‘my child was not like this before the vaccine’, and the male doctor and the male medical establishment silence her.
The Cult of the Needle
Vaccination is nothing but an invention of the most dogmatic religion ever known to man. That religion is science, shall we say, science of a most specific kind. Not science in the sense of gathering of evidence and a critical mindset, but science as conquest. And not religion in the sense of spirituality, the perception of the Divine, or any such thing, but religion in the sense of a formal doctrinaire belief beyond question.
That science and that religion exist as a crude, one sided reduction of reality into terms that can be written in a slogan: ‘Vaccines save lives’, ‘Vaccines are safe and effective’, ‘Without vaccines we would all die of measles/polio/Covid’. Vaccines are not science, because vaccination never has to prove itself scientific. The crude, ridiculous, absurd, notion of vaccination – the fundamental lie – that needle = antibodies = protection – cannot be scientific in any sense other than that of the most vulgar scientism. That these antibodies exist is in itself considered proof of faith. No-one has to prove these antibodies mean anything – we found them, so that means vaccination works. Even in the absurd case with Covid – where the manufacturers stated that these antibodies are not a proven established correlate of protection – the vaccinal antibody is exalted as the ultimate evidence.
The Vaccination Cycle of Abuse
As vaccination spreads throughout society, becomes the norm, the accepted, the beatified, so develops the vaccination cycle of abuse. Those that are vaccinated as children become damaged by that vaccination. The toxins in the vaccines enter the brain and begin to wreak their havoc.
What happens to these people? I am not talking about those killed or severely maimed by vaccination here, but rather those who go on to have somewhat normal lives. They help to build the vaccination-industrial complex you see around you. They go to work in the hospitals which promote vaccination. They go to work in the schools that promote vaccination. They go to work in the GPs’ offices that dole out vaccination. They go to work at the universities that produce scientific papers justifying vaccination. They work at the Pharma companies that produce vaccination. They work at the banks that finance the vaccine companies. They work at other businesses involved in the supply chain of goods to these industries that promote vaccination, and more and more, with ‘covid’ directly promote vaccination themselves. They donate to charities that promote vaccination in developing countries. They vote for the politicians that promote vaccination. Their taxes fund vaccination. Their pension funds invest in vaccination. And most of all, they perpetuate the vaccine crime against their own children. Everyone who lives in Vaccine Society contributes to the perpetration of Vaccine Society, to a greater or lesser extent.
The collective immorality of this system in itself helps to sustain it. That something is so normalised makes it hard to believe that it could be so depraved. But it also binds us together by guilt – to take part in it is to be guilty – even to the extent that one has no choice to survive in the world. The people working in the healthcare institutions – the people who have the potential to see the most harm from vaccination – are those most intertwined with the guilt of producing the damaged goods on the vaccine conveyor belt, those who are most indoctrinated into the vaccination cult. A mixture of factors sustains this: denial being one of the most important. Some see it, but live that contradiction. Maybe they don’t directly give vaccinations and justify that their role in the system does more good than harm. Or perhaps it’s just self interest – everyone knows that questioning vaccines simply isn’t good for your career – and damn, years of your life went into making that career. For some, it is pure sadism, gratuitous pleasure in the cycle of abuse. And some will quietly exit, seek ‘oblivion in suicide’1 when they can no longer bear their role as society’s perverse god. Only a small number leave the mainstream medical profession and speak out and accept the demonisation of society.
To the extent that there is any hope for humanity the only solution can be vaccination abolition. The cult of vaccination must be broken.
Unfortunately many are still lost in the cult, and with the mRNA ‘vaccines’ and the risks of that poison getting into the germ line (we know it congregates in the gonads) that makes any task of saving humanity from this madness ever harder. It may already be too late for an unpolluted humanity to exist outside of Africa, which is very lightly ‘vaccinated’. In fact I think any salvation may rest on how many of those doses were saline (or so degraded to produce no mRNA biological effect) – I know there has been a large amount of speculation about this question. I take no position though the clear difference between batches and reported ‘vaccine’ injuries does prove that some doses are more dangerous than others (but doesn’t necessarily prove that the less bad batches contained saline or extremely degraded product). The possibility that babies from birth are spike protein factories as induced via their mother’s ‘vaccination’ for Covid is utterly horrifying but the idea must be broached. There could be other effects induced via the lipid nanoparticles as these could affect the ova and sperm in the gonads (even upon the theory that the Covid virus doesn’t exist although if that theory is true we are in a stronger position).
What must we do?
The first thing we have to do is look at ourselves. Obviously, we need to decline and reject every single vaccination for ourselves, our children. But much harder than this, we need to try and walk away from the system as much as possible. No-one can avoid some complicity in the system unless they are willing to starve to death. But you need to try and position yourself in a job role where you are doing the least amount of harm and have the least amount of complicity possible in vaccination. Certainly the vast majority of people working in healthcare – any mainstream medical institution – should leave and refuse complicity in the system any longer. If you donate to charity, you should stop, although I imagine that most people reading this don’t. This is because charities claiming to do good work abroad promote and push vaccination, and pretty much all of them promote the Covid ‘vaccine’. Many of them, such as National Autistic Society or Alzheimer’s Society, exist to normalise the effects of the poisoning we undergo. Even pet charities promote pet vaccination. There may be local/smaller groups that are an exception to this rule but the larger ones probably should be avoided.
The harder part is accepting our pariah status. The above things can be done quietly. If you talk about this issue you will become a pariah. There is no other choice. So psychologically prepare yourself for that role. Many people, of course, have already experienced this pariah status via their objection to the Official Covid Narrative and so are prepared to take their pariah status to the next level by becoming fully anti-vaccine. We must get as many of the people who questioned the Covid ‘vaccine’ (whether before, or after, taking it) over to the fully anti-vaccine side. People who have children and did not inject them with the Covid poison are top of this list (in order to protect the children from other vaccinations – sadly those fanatical enough to inject their children with the Covid shot probably cannot be saved. I want to save all children, of course, but I don’t have a practical solution on this point).
As for healing from vaccination damage? Of course, we should try to bend societal resources towards real help for the vaccine-injured. But for some of us, it is already too late. The poisons have already wreaked too much havoc, we are already too damaged to live in a sane, post-vaccine society. We cannot relate to healthy humanity, nor do we understand it. So the war cannot be for ourselves. It is for those for whom it is not too late, whoever that remains to be.
Thomas Szasz’s phraseology in The Manufacture of Madness, discussing the high suicide rate among psychiatrists. “The oppressor [becomes] a megalomanical, godlike figure. Once [the psychiatrist realises] that he is but a mockery of God, the result is often explosive violence…the victimiser [seeks] oblivion in suicide.”, Syracuse University Press, 1970, p. 41. Doctors are known to have a higher suicide rate than the general population. Mainstream opinion puts this down to higher exposure to death due to the profession. While death desensitation plays a role in suicide, in my opinion, Szasz’s theory is closer to the mark.
Image Source: Photo by Nataliya Vaitkevich on Pexels.com
Vaccination is considered by mainstream society to be a scientific practice, with no other motivations behind it other than those based in evidence. However, vaccination is not actually a scientific practice, but a cult practice, and this article will outline the reasons why vaccination can fundamentally be considered a cult.
I. The Promise of Salvation
All cults begin with the promise of salvation. The promise of salvation in the vaccination cult is the eradication of that we most fear: disease and death.
Death is humanity’s biggest fear, broadly speaking. It’s fair to say that this applies to most human beings, although there are exceptions to this rule. Disease and illness is also another large fear, that we will become ill and will be unable to care for ourselves and our families.
Vaccination offers to remove all our fears and doubts about death and disease. It offers what I would call the ‘Fantastical Conquest of Disease Narrative’, as a means to eliminate this fear. This narrative goes something like this:
In the time period Before Vaccination, people were constantly dying of disease. There were deadly outbreaks of diseases like smallpox which killed millions. Then Edward Jenner invented to concept of inoculation via cowpox, and soon the Smallpox Vaccine would come to save millions of lives. As the Industrial Revolution progressed, and science developed more and more, more and more life saving vaccines were developed. Because of this, disease plummeted. Vaccination is the reason that we have a good quality of life today and don’t have to worry about our children dying from measles, etc. Now, After Vaccination, we have our salvation.
II. The Receipt of the Salvation Ritual
However, in order to gain salvation, one must submit oneself or one’s children to the receipt of the Baptism of the Injection.
The receipt of the injection is a cult ritual. It is a sacred act. One is prepared for the receipt of the injection by the doctor, the modern day priest. The clean sterile environment, free of danger, germs, serves like the stained glass of old – to induce reverence, and as a reminder of what bounty one (or one’s child) will receive for undergoing the pain of the needle – a sterile, germ free body. Like the priest, the doctor reassures, soothes, it will all be over soon like an awkward session of confession. It is to save one’s body like confession is to save one’s soul. Sleeves are rolled up, skin prepared, pricked, plungers pushed. Maybe the child cries: he does not understand this is to save him. The doctor puts a plaster on it. There, all done, all over, the ritual is completed. There are lollipops, see, to soothe the pain.
To inject one’s children with vaccines is to induct them into the cult of vaccination, and this is the societal function of paediatric medicine. The whole function of institutions such as baby check ups is to establish compliance with the cult rituals of vaccination and ensure all doubt is removed from the parents’ mind. The indoctrination of the broader society into the narrative that vaccination is always good, via the media and government, is pervasive, but there may still be some parents who have questions. Perhaps something broke through to them on a social media platform, perhaps they heard another parent talk about suspected vaccine injury in their child. Doubts cannot be allowed to fester, they must be smoothed over with the concrete of authority to fill in the cracks. You see, the doctor knows best.
The Covid-19 Narrative has allowed for even adults to themselves confess their faith in Vaccination via the Covid-19 ‘vaccine’ products. Prior to Covid, adult vaccinations were not all that important – even the flu shot, which is pushed to an extent, did not reach the sanctity of the childhood vaccination schedule. With Covid, adult vaccinations became fundamental. An adult must not only confirm their faith by injection of these products into their children, but receive them personally. And so many followed suit! Not only did they receive the holy ritual of vaccination, they openly expressed their reconfirmation of faith in vaccines on social media. How many selfies with ‘I’ve Had My Covid-19 Vaccine’ did you see? How many images of a masked, presumably smiling face, with a white-coat hovering over them pushing a plunger? The constant receipt of Covid ‘boosters’ – indicating the failure of the initial series, else why would ‘boosters’ be required – also serves as a reconfirmation of faith.
Vaccination also gives meaning to people’s lives. No doubt the quote above is an exaggeration – I’m sure there are atheists who question vaccination – it nevertheless makes an excellent point. The decline of traditional religion has meant that people do not have meaning in their lives, and even more so with the mass modern atomisation of traditional communities. Preaching the Gospel of Vaccination – like so many scientists, bureaucrats and general do-gooders do – provides a helpful alternative to create that meaning.
In general, those that are opposed to vaccination are seen in a negative light – and there are two categories of such people: The Hate Figure (more on hate figures below) and the Ignorant (who concern us here). The Ignorant are seen as needing education from the white-coat about vaccination, as being too stupid to understand, and they just need to accept the offer of salvation from the white-coat. In the Western internet age these people are often seen as dupes of evil, malicious hate figures – i.e. the main spokespeople of the anti-vaccination movement, who in a tremendous example of projection are only out for money.
There is also a large aspect of a White Saviour Complex to this narrative, with ‘ignorant’ Africans needing to be educated by white Westerners about vaccines, so that they can be ‘saved’ by the receipt of the injection. Any institutions that stand in the way of the delivery of more vaccinations in any African country – such as on occasion the Catholic Church – are demonised regardless of the truth of their claims or legitimacy of their questions about vaccination.
Any questions about vaccination are dismissed as ‘reactionary’, ‘right-wing’, ‘anti-science’ – these simply stand in the way of ‘progress’, progress defined as shiny tip of a needle.
IV. The Apostate as Hate Figure
One of the most notable features of a cult is that it cannot tolerate dissent, and must silence any critique. One method how this is done is the creation of a hate figure – a person who represents what the cult does not.
When it comes to the vaccination cult the most notable hate figure is Dr. Andrew Wakefield. The Official Narrative, repeated ad nauseam in the mainstream media, is that Wakefield is a disgraced, immoral fraud. The endless repetition of this narrative provides a hate figure for believers in the vaccine cult to pour their wrath upon. Like the Two Minutes Hate in 1984, this hatred reinforces the belief in the narrative. But the hate figure can also act as a balm for the reason why vaccination has not achieved its salvation promise of elimination of disease and death. We see this whenever there is an outbreak of measles or mumps anywhere. Because of Wakefield’s criticism of the MMR vaccine, he gets the blame. There was an outbreak ‘because disgraced British doctor Andrew Wakefield convinced parents with his lies not to vaccinate with the very safe MMR vaccine’, not because of any problems with the concept of vaccination or the vaccine program. The truth is irrelevant, the target is set, and any questioning of the cult is cut off.
And of course the most obvious reason for the creation of a hate figure is to inculcate fear – to make someone questioning the cult think twice about leaving, lest they be demonised and lose their career and income. This serves to keep any other doctor in line who might think about questioning vaccines. Fundamentally, Dr. Wakefield fits the role of cult apostate: he (and prior to him, members of his family) trained in the mainstream medical system – one of the pillars of which is the worship of vaccination. Thus his trial before the General Medical Council and by media, and his eventual striking from the medical register, should be seen through the lens of excommunication.
Conclusion
The four aspects outlined above serve as the basis for the establishment and maintenance of the vaccine cult in society.
I don’t usually put out short commentaries/news type posts as I generally like to keep the blog as a place for long posts or protest coverage. However in this case, this news story is so worthy of note, and I have seen very little on it out there so far, and I am so angry about it, that I am making an exception.
The media today in the United Kingdom have just reported the below story, headlined:
The 32-year-old, who can’t be named for legal reasons, spent lockdown in his room at a care home because his parents refused to let him be vaccinated, Jersey’s Royal Court heard.
To translate this from mainstream media bullshit to English, the care home locked him in his room because his parents did not want him to be harmed by a ‘vaccine’. When he had already been harmed by vaccines. His parents should have had him removed from the care home, if possible, although some of these care homes have put obstacles in the way of getting people out and I don’t know if that’s the case here.
Jersey’s Royal Court granted the vaccination order, saying that it was ‘the right best interests decision’ for B who had been in ‘groundhog day’.
In other words, this man is stuck because the care home won’t let him out because he’s not jabbed so they want to force him to be jabbed. When they could get rid of the problem by simply not treating him as subhuman for not being jabbed.
This also involves denying him treatments, according to the Times:
He is not able to attend the treatments, such as hydrotherapy, which soothe him, or the ones that cheer him, such as watching the Christmas lights being turned on, stuck in what his nurse describes as a “shrunken world”.
2021 has been the year in which human beings have been subjected to the most intensive, most obsessive, and most outright nonsensical propaganda campaign in human history.
So how has that propaganda campaign held up in 2022? Fortunately, it has has been forced onto the back foot, at least to a degree. There have been victories against the narrative here in the UK, such as the NHS ‘vaccine’ mandate being rejected, the care home worker mandate being repealed, and no more lockdowns. Over here at least, there is only a small percentage of people still wearing a mask, and although the media does its best to fearmonger about Covid, people aren’t buying it any more.
On December 19, the most recent date for which reliable figures are available, just 14 Stoke-on-Trent residents were vaccinated – with one person receiving a first dose, three getting second doses and 10 booster or third doses.
There are, of course, still covid fanatics out there but they are becoming a minority.
The Bad News
There are however, new threats on the horizon. As I have said before, the point of the Official Covid Narrative is not the narrative itself. The point is to use the narrative to drive in an authoritarian, technocratic, transhumanist mass surveillance dystopia via digital IDs, Smart Cities, and Central Bank Digital Currencies. They can do this without Covid, for example, through narratives of ‘saving the planet’ or terrorism (the main narrative used to push mass surveillance prior to the Covid scam).
One of these threats is currently being pushed in Oxford:
Road blocks stopping most motorists from driving through Oxford city centre will divide the city into six “15-minute” neighbourhoods, a county council travel chief has said.
While this will be promoted as ‘saving the planet’ it is actually a form of controlling people’s movements, and will be used to normalise checkpoints through which you cannot pass if you are not the ‘right’ kind of person (whether that’s to do with ‘carbon credits’, ‘vaccination’ status, or political opinion) no doubt connected to one’s digital identity.
But there is something even more important that is worthy of discussion. The horror from this year can be summed up in two words:
Died Suddenly.
Those two words used to normalise mass deaths from the mRNA injections.
So let’s talk about died suddenly. ‘Died Suddenly’ is, in a large percentage of cases, a media euphemism for mRNA injection induced death. This largely but not entirely replaces its previous role as a euphemism for the manner of death for those that have killed themselves.
We have plausible mechanisms of mRNA ‘vaccine’ induced death. Even governments have admitted that these injections can damage the heart.Blood clots are another harm admitted by the establishment. There is significant evidence of myocarditis, pericarditis, stroke, blood clots, cardiac arrest, and heart attacks being caused by the injections – and these can lead to death.
So we have our deaths, our correlations, our mechanisms. But what I wanted to get to was the tsunami of news stories about those who ‘died suddenly’.
For the last few months, I have been working on the ‘In Memoriam of those who ‘died suddenly” project as started by Mark Crispin Miller. The project is a long compilation of deaths all around the world, posted every week, of those who ‘died suddenly’, often with no cause of death listed, or from the above listed causes that often indicate that ‘vaccination’ was involved in the death. As a result, every day I am searching for evidence of people who ‘died suddenly’ for this project.
I have my reasons for taking on this burden of death – to document this crime-in-progress of mRNA ‘vaccine’ mass murder, and other reasons and motivations I won’t get into. My experience doing this project is that it is everywhere. I focus mainly on countries with Russian-language media and Asian countries as well as the UK to a degree, but cases of people dying suddenly pop up from all over the world – either with no cause of death, or the telltale ‘cardiac arrest’, ‘blood clots’ or ‘stroke’ listed.
While the cases of young people dying of these conditions – which rarely affect them normally – are the most striking evidence of mRNA murder – we should not lose sight of the fact that this is a truly universal phenomenon. Male, female, black, white, Asian, old, young, middle aged, Western, Eastern – none of this matters. There are people in all these categories who have been killed.
People who aren’t watching this as closely as I am may not grasp the full implications of what we are witnessing. I’d like to offer some observations based on the reports I have found over the last four months:
Heart Attacks and Cardiac Arrest seem to be rampant in the 40-65 age demographic. Perhaps a slightly overlooked fact, given the more shocking cases among under 30s and sometimes teenagers.
There are a large amount of videos of people just dropping dead. Particularly from India. They are doing a normal activity like dancing and just drop.
There’s also a large amount of testimony of people just collapsing, having been fine the moment before, for example, I have found Russians dropping dead at bus stops.
I don’t believe we are getting anywhere near close to the death toll with the ‘Died Suddenly’ project. Obviously, a large number of cases are never reported anywhere. But even on top of that, there must be news articles that are never found that belong in the project. Most of the Russian ones are reported on local news media websites, for example. If one had the time to check Russian-language local news media across the whole country I reckon a lot more deaths would crop up. But no-one can feasibly manage that. Plus there’s cases excluded from the project due to ambiguity about the cause of death that may have been ‘vaccine’ related.
None of the media in any of the countries I have researched acknowledge there is even a problem, with the exception of India. Indian articles will sometimes state ‘There have been a large number of heart attacks recently’, or, ‘There have been a lot of people dying suddenly dancing at weddings, etc.’ In most cases they don’t blame the ‘vaccine’ but I have seen a couple of examples where the journalist, or who the journalist is quoting, question the ‘vaccine’.
The media is trying to blame anything but the ‘vaccine’ for these deaths, when it does acknowledge that the death was unusual more specifically. Blaming Covid is one strategy, blaming cold weather (or other random factors) for heart attacks instead of the ‘vaccine’ is another strategy. The nebulous ‘Sudden Adult Death Syndrome’ is another one.
When this fails the media accuses ‘anti-vaxxers’ of ‘weaponising’ the deaths of famous people by asking questions. I remember reading one comment that referred to us as ‘grave robbers’, showing disrespect to the deceased. Of course the true disrespect to the deceased is to refuse to ask these questions about what may have killed them.
Being honest, I don’t think this situation is going to improve, I think it will continue or get worse. Even if all ‘vaccination’ stops now, too many people have been damaged, as Dr. Peter McCullough has outlined, with subclinical heart damage that will lead to sudden death. This is where they have led us, where they watch the people that trusted them die. Us dissenters who did not take the injections – unless they resort to more extreme methods – are going to live, but what are we going to live with?
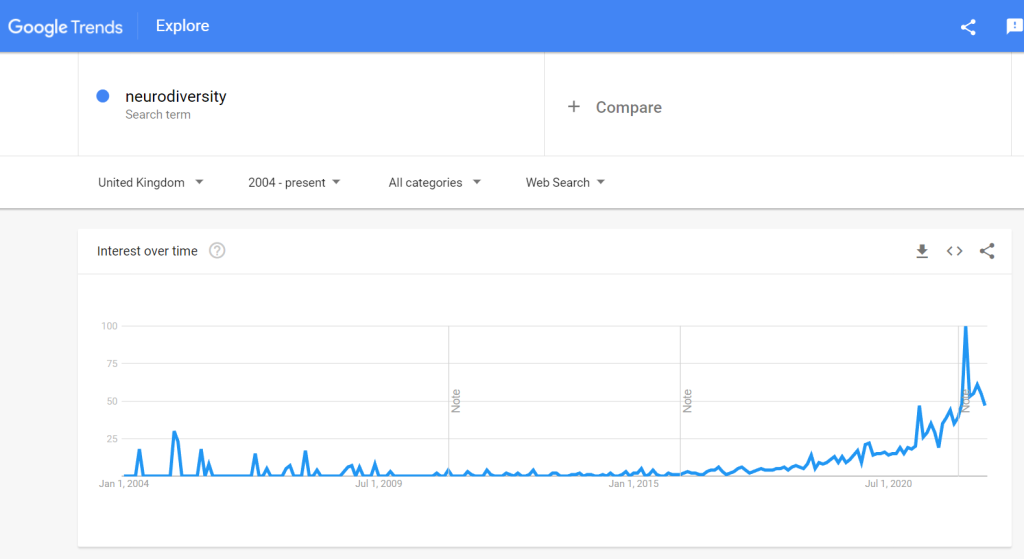
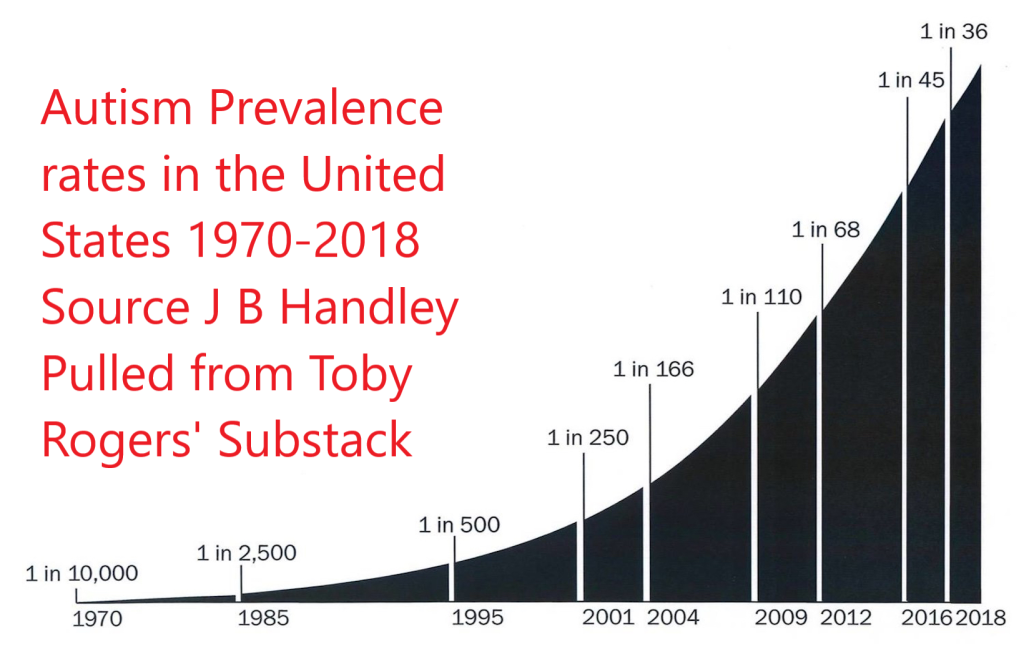



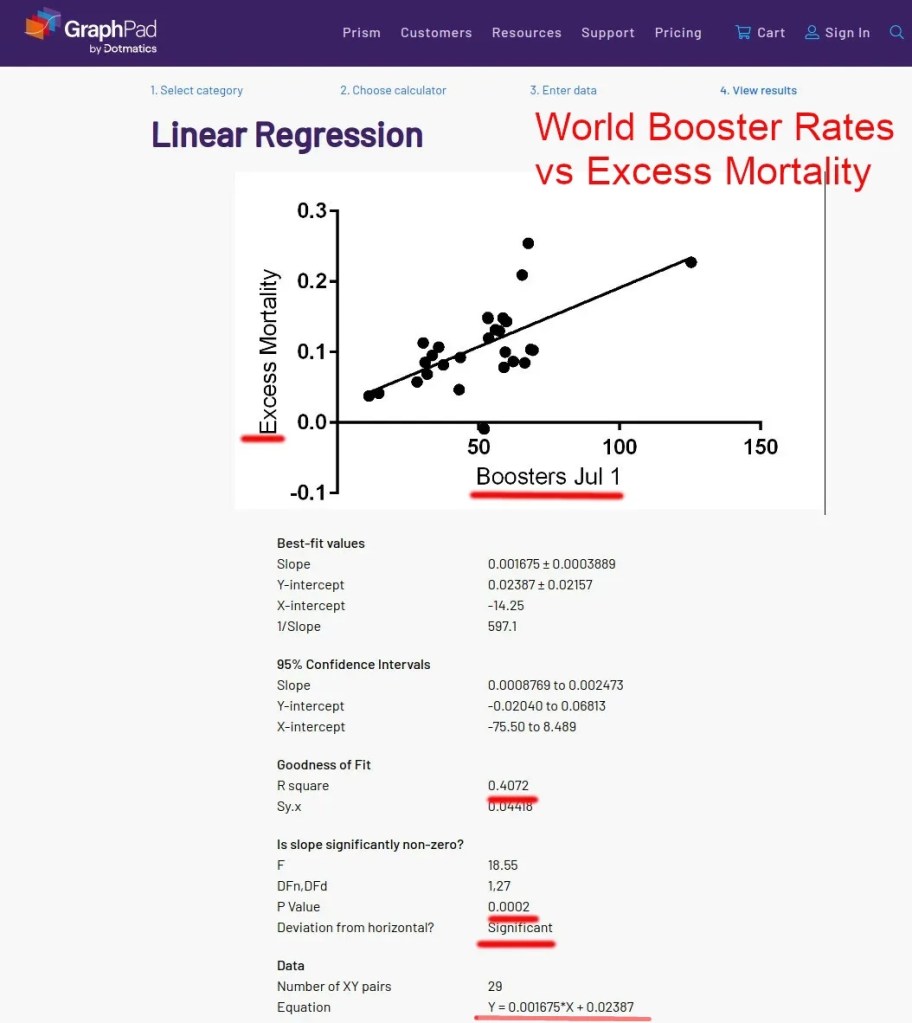
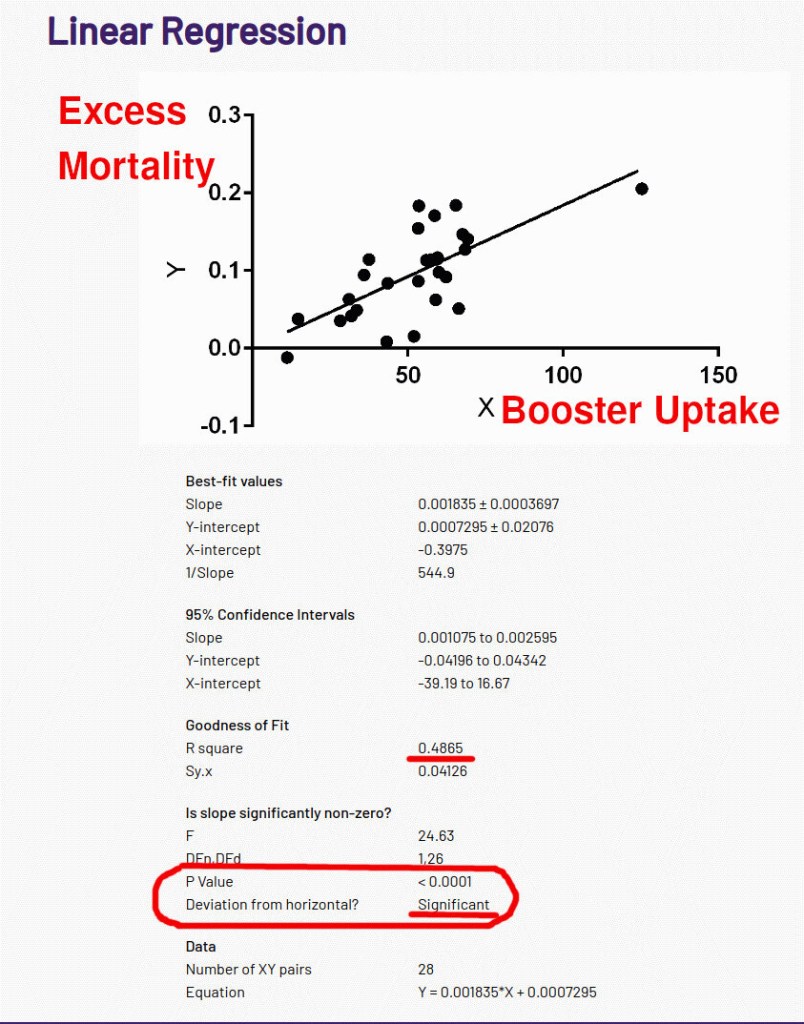

{kind=link}