The concept of death is often invoked in the discourse of allopathic medicine. This is for the obvious reason that medicine is concerned with issues of life and death on its face. However, death is also used as a discourse in cases where it has no particular relevance: the patient in question does not have a life threatening disease. In these cases, death is evoked as a means to get a parent or patient to comply with the doctor’s desires for treatment. This is seen in two specific cases: transgender ideology and vaccination.
Death in Transgender Ideology
Transgender ideology is based upon the idea of gender identity. The theory of gender identity claims that an individual’s ‘gender’ can be different from their sex. There is more than one theory about how this works among gender ideologues. One theory says there are only two ‘genders’, man and woman, but that either sex can identify as either gender. The other theory states that there are all kinds of different genders apart from man and woman. These gender identities impose costs and obligations on other people, as people are expected to use pronouns in line with the other person’s identity as well as believe that a man is actually a woman and vice versa.
The transgender phenomenon is a boon to the medical profession. The provision of opposite sex hormones and imitation surgeries provides a large source of profit for pharmaceutical companies. It creates whole specialties for doctors and surgeons to work in, and allows them a tremendous amount of power over human bodies. They get to play at attempting to create whole new sex organs and come up with their own bizarre combinations. As such they have an incentive to promote this ideology, particularly to those who will be vulnerable to accepting it.
As such, parents of underage children who identify as transgender are a significant target for this kind of manipulation. They are generally suffering from a large amount of confusion regarding their child’s declaration of their identity. They often do not know how to react. Sometimes parents have an innate suspicion of the extreme measures suggested by the gender ideologues, of puberty blockers, hormones and surgeries. This is due to the permanent nature of the intervention, as well as the fact that teenagers especially often have identity issues that resolve over time without any help. As there is a connection between the autism epidemic and transgender identity, parents also often consider that their vaccine injured children are being manipulated due to poor social skills.
Doctors advocate transgender hormones and surgery as the only option for these children and teenagers who declare a transgender identity. This is regardless of the possible cause of the declaration. In doctors’ minds, there can only be one cause, that the person is truly a ‘different gender’ and that is the cause of the declaration. However, in order to get wary parents to go along with the medical intervention required they need a stronger justification than this.
This is where the threat of death enters the picture. Suicide is considered to be an almost inevitable result of refusing to accept an individual’s self declaration of identity. The idea is often put to parents of ‘would you rather have a live daughter or a dead son’ to emphasise the inevitability of suicide without medical intervention.
Death in Vaccination Ideology
Vaccination ideology states that death from infection was rampant before vaccination, and only vaccination has been able to tame it. Vaccinationists dismiss all other context as irrelevant. For example, they ignore diet and access to food, sanitation or the lack thereof, economic factors, etc, in death rates from disease.
Doctors and scientists advocate vaccination in every and all circumstances, and they obviously gain large amounts from vaccination. This includes financial gain from both vaccination and treating vaccination injuries, whether this is direct via profits from vaccines or indirect via the higher demand for the service created by vaccination or injury. Doctors are also strongly ideologically committed to vaccination.
As such, they seek to get people to take vaccines, and parents are the main target in the promotion of vaccine ideology. However, some parents have concerns about vaccination. These concerns can range in scope and scale and can include belief that a specific child should not receive a vaccine due to individual sensitivity as well as criticism of vaccination in general. Concerns can involve: belief that a vaccine causes injury, particularly autism; belief that the amount of vaccines on the childhood schedule is excessive; or concerns about certain ingredients in vaccines such as thimerosal or aluminium (this list is not exhaustive).
Doctors deal with these concerns by invoking the threat of death. A parent is told that their child is at very high risk of death should the parent decline vaccination. Diseases where there is a vaccination are portrayed as equally deadly regardless of context. In some cases, the fact that the disease had a high death rate in times past, or has a high death rate in developing countries, is used as evidence for the current risk.
The media also covers stories where they allege that children died (or became disabled) due to lack of vaccination. Usually in this type of media story the parent is portrayed as being repentant and regretting not vaccinating.
Conclusion
Both transgender ideology and vaccination ideology seek to control people using the fear of death. In particular the fear a parent has over the death of their child. They grossly overexaggerate the risk to a child of not taking a particular medical intervention. In fact, there are plausible arguments that both of these medical interventions are more likely to directly or indirectly cause death than prevent death.
Both these ideologies also offer a form of illusory control over death, which is an attractive proposition to parents who fear the death of their child. Transgender ideology states that a child’s suicidal tendencies can be checked if only they are fully accepted. When this fails, perhaps due to the medical abuse inflicted on the child, it can simply be claimed that they were not accepted enough. Vaccination seeks to abolish disease via the needle. If disease is not abolished, it is the fault of antivaccinationists. The main difference between the two ideologies is that vaccinationists seek to blame a child’s unvaccinated body for death in other people, whereas in transgenderism the blame is only for self-inflicted death.
This series hopes to explore the history of British Antivaccinationism and Vaccine Scepticism. It is divided into 7 main eras: the period of Inoculation, 1721-1798; the introduction of vaccination, 1798-1853; the imposition of mandates, 1853-1902; the remaining history of the National Antivaccination League, 1902-1972; DTP Vaccine Scepticism 1972-1998; Andrew Wakefield and vaccines cause autism, 1998-2019, and Covid 19, 2020 to present. This section forms part 2 looking at Jenner and his critics.
The ‘Discovery’ of Edward Jenner
In 1796, Edward Jenner performed his first vaccination. This was on an 8 year old boy called James Phipps. In this experiment, Jenner inserted into the arm of the boy matter from the teat of a cow with cowpox using a lancet. Cowpox was a disease of the cow’s udder, which caused pustules to appear on that area. It was transmitted to humans via the action of milking a diseased udder.
Jenner’s justification for doing this was that cowpox allegedly prevented smallpox. There had long been a rumour among dairy maids that they could not contract smallpox, if they had contracted cowpox. In fact, the official story or mythology of Edward Jenner states that he overheard this idea from a dairy maid when he was a teenager and was taken with testing it (this is narrated by Jenner’s sycophantic biographer, John Baron).
Jenner became a country doctor in Berkeley, Gloucestershire. He became a member of the Royal Society after writing a paper about cuckoos that was accepted. In 1796, when Jenner performed his first inoculation with vaccine virus (later known as vaccination) he wrote a paper outlining his theory of the origins of cowpox (he believed that it originally came from the horse, and was transferred to the cow via those who dressed diseased horse heels). He then outlined the theory that the cowpox infection prevented the smallpox infection. He used some examples of those he met in his practice who had had a cowpox infection, on whom inoculation (deliberate infection with smallpox) would not ‘take’. The failure of inoculation to take was interpreted as immunity to smallpox. He also outlined his test on James Phipps, first inserting cowpox matter and several weeks later performing inoculation on the boy. As the inoculation did not take Jenner interpreted this as proof of immunity.
The Royal Society rejected Jenner’s paper. They believed it did not have enough evidence to support it and that it might tarnish Jenner’s reputation. Jenner was still determined to publish, so he added more evidence – increasing the number of cases of vaccination. (A detailed discussion of the differences between Jenner’s first and second versions of the paper can be found in Crookshank’s book). He published it in 1798.
Pearson and Woodville
Two important figures took up Jenner’s vaccination idea, George Pearson and William Woodville. Both these doctors were vital in spreading the practise of vaccination and backing it ideologically.
William Woodville was the lead doctor at the Smallpox Hospital in London, so it can be imagined that he had significant influence over the treatment and prevention of smallpox. He took to the idea of vaccination and ran a significant number of tests. Woodville’s tests had many flaws, in particular that he sometimes attempted cowpox and smallpox inoculation very close together. However his testing was more extensive and better documented than Jenner’s.
Pearson sought to set up an institute for vaccination. This annoyed Jenner, as he was not consulted in advance regarding the project. Pearson also distributed vaccine lymph early on in the process to allow other doctors to perform vaccination, which was important as Jenner did not have vaccine lymph to give out on many occasions.
Jenner had a significant number of supporters in the medical profession. When he was put forward for a government reward in 1802, a large number of doctors spoke in his favour. The profession adopted Jenner’s theory very quickly, and it spread widely. This included across Europe, the United States, as well as many colonised countries.
Jenner’s Critics
Jenner had three main critics of his theory when it was first published. These three men were Benjamin Moseley, John Birch, and William Rowley. None of these men were antivaccination in the sense that we would understand this term today, i.e. they were not opposed to all artificial inculcating of disease. They were supporters of the old method of inoculation and sceptical of Jenner’s attempt to replace it. At this time, there were no high profile critics of both inoculation and vaccination (this tendency would only develop post vaccination mandate, from 1853).
These three men opposed the award to Jenner by the British government during the hearing on this issue in 1802.
Benjamin Moseley
Moseley was a doctor who was well known for other writings prior to his involvement in the vaccination controversy, in particular writings relating to the Caribbean.
He opposed Jenner’s method early on, and published more than one book relating to the issue. He considered that a ‘cowpox mania’ had taken over the medical profession. In his book, A Treatise on the Luis Bovilla, Or Cow Pox, he made several arguments. He stated there was no affinity between cowpox and smallpox, so there was no specific property of cowpox which meant it could prevent smallpox. He also argued that cowpox was not necessarily a mild disease. He pointed to the ulceration that often accompanied the practise.
John Birch
John Birch was a surgeon who was opposed to vaccination. In his text, Serious Reasons for objecting to the Practice of Vaccination he discusses the Royal Commitee on Vaccination. He argued that there was a large number of vaccine failures but that most of these were not admitted, and that the Committee tried to soften the language by stating that these cases only apparently had cowpox.
William Rowley
William Rowley was an active practitioner of inoculation. As such it could be said that he had a degree of vested interest in defending the practise against the new threat of vaccination. He considered inoculation to be a very safe practise that rarely led to death when performed competently. Vaccination, on the other hand, he considered both dangerous and ineffective.
Rowley authored a work called ‘Cow Pox No Security Against Smallpox Infection‘. This book has been considered a target of mockery by vaccinationists due to a couple of the images included in the book. These images claimed to show vaccination injuries, but as Rowley had titled one of them ‘The Ox Faced Boy’ he was mocked for making a linkage between vaccination and people becoming bovine.
Rowley actually collected a large number of cases, including with address details so at the time they could be checked, of vaccination injury, death, and cases of smallpox after vaccination.
He also provides an extensive list of excuses used by vaccinationists to defend their theory. These included the theory of ‘spurious cowpox’, which was outlined by Jenner in his second essay on cowpox. The idea of a ‘real’ and a ‘spurious’ cowpox allowed any cases of failure to be assigned to a spurious vaccination. He also accused vaccinationists of misdiagnosis of cases of smallpox in vaccinated people. He also states that vaccinationists formulated the excuse that even if cowpox failed to prevent the disease, it made it milder.
Conclusion
Vaccination had some significant opposition. However, it is fair to say that it had very little ideological opposition at this time. Its opponents thought it was unsafe and ineffective but advocated the earlier practise of inoculation instead rather than rejecting both. Well founded ideological opposition to vaccination would have to wait until after 1853 – the year of the UK’s smallpox vaccine mandate.
This series hopes to explore the history of British Antivaccinationism and Vaccine Scepticism. It is divided into 7 main eras: the period of Inoculation, 1721-1798; the introduction of vaccination, 1798-1853; the imposition of mandates, 1853-1902; the remaining history of the National Antivaccination League, 1902-1972; DTP Vaccine Scepticism 1972-1998; Andrew Wakefield and vaccines cause autism, 1998-2019, and Covid 19, 2020 to present. This section forms part 1, looking at the inoculators and their critics.
The History of Inoculation
Inoculation was the practise of deliberately infecting someone with smallpox. The theory behind the practise was that a person could only get smallpox once, and would then get what we would call natural immunity. Although this concept was not understood, it was observed that smallpox was only contracted once. As such, by selecting the time and place of infection, and by carrying out additional practices such as the following of certain diets, smallpox could be rendered a milder disease with a greater chance of survival.
Lady Mary Wortley Montagu observed the practise of inoculation in Turkey and had one of her children inoculated while over there. She introduced the practise to her physician, Charles Maitland, who was taken with the idea and began to practise inoculation on willing members of the elite. There was a brief fad for this practise initially, but the first wave of enthusiasm died out quite quickly, and the number of inoculations performed was still very small. Some doctors tried to collect scientific data relaying to inoculation, such as Jurin, who attempted to figure out the death rate from inoculation versus the death rate from natural smallpox infection – he calculated it at about one in 50 for inoculation versus 1 in 6 for the natural disease. On this basis, he argued for the supremacy of inoculation but acknowledged that it had some risk.
Inoculation became more widely practised later on in the 18th century and particularly in the second half of that century, with the rise of the Suttonian method of inoculation, which was less harsh on the body. Daniel Sutton was able to widely promote his method among elites, and inoculation became more popular. The Suttonian method was that in practise before it was replaced by the cowpoxing method associated with Edward Jenner.
The Masseys – The Original Anti Vaccinationists
In response to the introduction of inoculation, two men, Isaac and Edward Massey, brought objections to the table against the new practise. They could be considered the original antivaccinationists. Each of the Masseys put forward a different approach to the issue.
Edmund Massey’s religious objections
Edmund Massey was a Christian clergyman at a church in London, and he objected to inoculation on religious grounds. He preached a notable sermon in 1722 against the new practise which was distributed in written format. The first argument he uses against inoculation is that it is forbidden for man to deliberately inflict disease. He states that while the Bible furnishes examples of men healing when given divine power, there are no examples of men directly inflicting disease. Instead, God inflicts disease to test people’s faith and to punish sin. He raised the book of Job as an example of this.
Isaac Massey’s scientific objections
Isaac Massey raised scientific objections to inoculation. He was an apocethary (which was quite vaguely defined but involved working in the medical profession). In his book, A Short and Plain Account of Inoculation, he raised several different scientific objections to the practise. For example, he claimed that those who were inoculated were not necessarily getting genuine smallpox. He pointed out that it was an uncertain procedure, despite the claims of the inoculators to the contrary that factors such as age and the time of year can be controlled.
He stated that inoculation was ‘a disease of their own making and procurement’. He argued that when true smallpox is spread by inoculation, it can also spread to other people, such as in the case of the inoculation of Mary Batt, which spread smallpox and led to the death of a servant. He argued for living a sober lifestyle as a means to reduce the risk from smallpox.
In his book addressing Jurin’s statistical claims, he argues that Jurin did not allow for factors such as age, disease and poverty when calculating comparative death rates. Most who would have been inoculated when Massey was writing would have been elites, who would have had a better rate of survival from natural smallpox due to more adequate nutrition and being less likely to live in complete squalor. He thus considered that Jurin was not comparing like with like. He also pointed out that inoculation may spread other diseases. He pointed out that the initial claims of the inoculators was that the procedure was harmlessly and that this had to be revised when deaths occurred.
Conclusion
The objections to inoculation did not prevent the practise from eventually becoming widespread in certain elite circles. Inoculation formed the ideological basis for Jenner’s much more well known vaccination practise.
One of the key aspects to vaccination is the aspect of ritual. The public practice and promotion of this ritual during the Covid-19 ‘pandemic’ shows some similarities with a previous public vaccination mass participation event: the Salk vaccine trials in the 1950s.
An Overhyped Disease
Without getting into the detail of what caused poliomyelitis (paralytic polio), whether it was the poliovirus, pesticides like DDT, both, or something else, the risks were generally overstated. If we go with the virus theory, the vast majority of people infected with the poliovirus had no symptoms even on the official version. For example, the NHS website states:
This was historically known as well. For example, an article published in 1916 states:
In a large aggregation of people, such as the population of a city with over 100,000 inhabitants, a county, or a State, epidemics seldom attack more than one in a thousand of the population, often not more than one in two to four thousand.
Objectively, many other diseases killed more people than polio did, even given that poliomyelitis could be fatal.
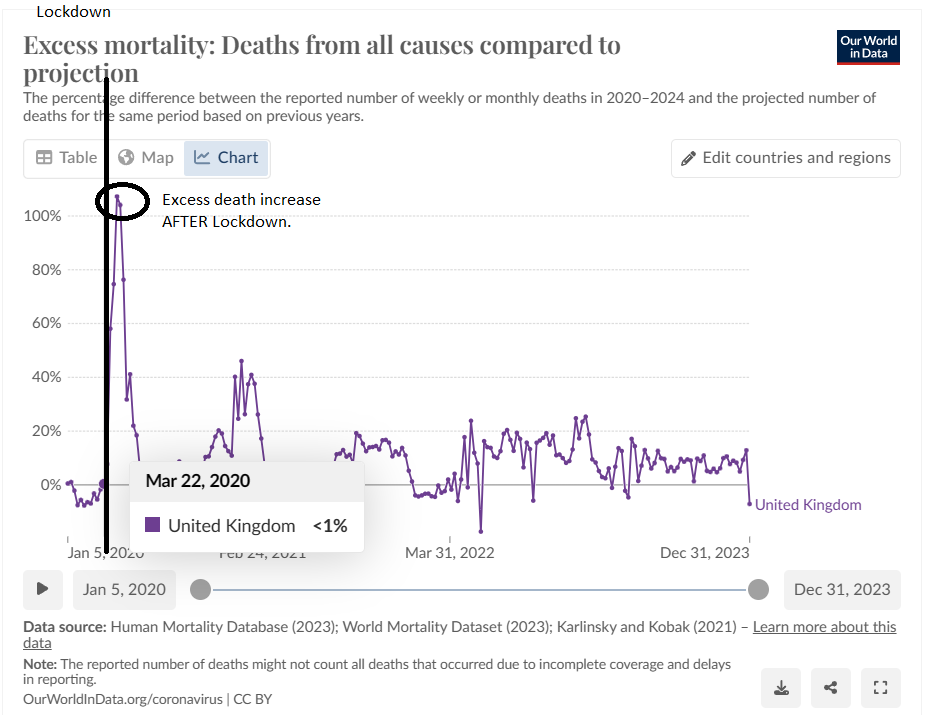
Covid-19 was also an overexaggerated threat. The government and media promoted the idea that Covid-19 was so dangerous that it justified lockdowns, forced masks and experimental ‘vaccine’ technologies. However, reality does not match that apocalyptic vision. In reality, excess deaths in the UK only increased after lockdowns were introduced, not before:
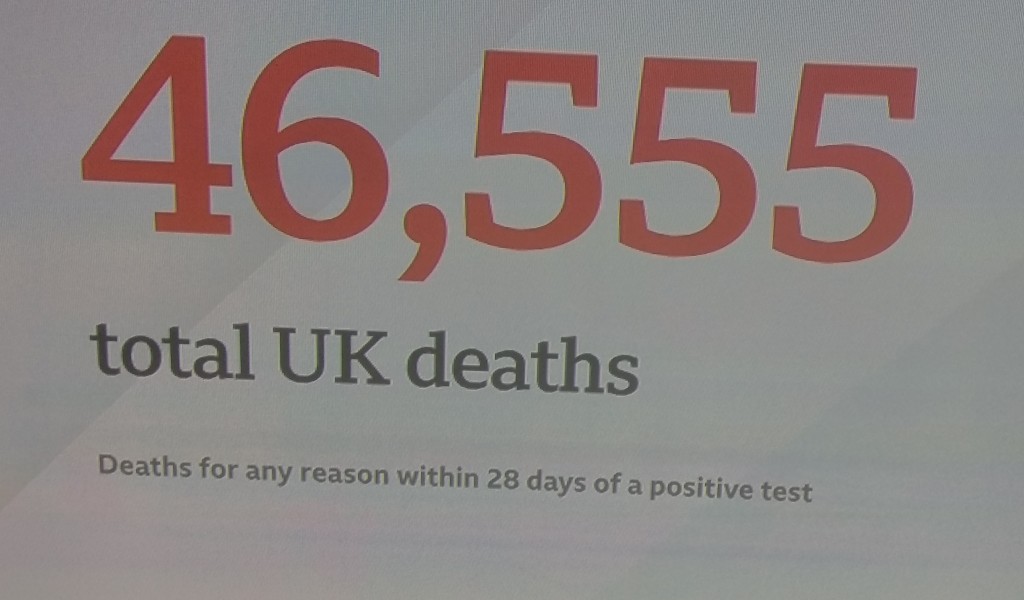
Unlike poliomyelitis, which mainly affected children, Covid-19 deaths were mainly among the elderly. It was rare for young and healthy people to die from Covid-19. The number of deaths from Covid-19 were exaggerated by media, by defining Covid-19 death as ‘death within 28 days of a positive test’ regardless of cause:
Science Saves the Day
In both of these cases, heroic vaccine scientists were portrayed as fighting the evil disease through their ingenuity. The key difference would be that in the case of polio, there was more focus on Jonas Salk, the creator of the first polio vaccine to be used on a mass scale, as an individual. Whereas, in the case of Covid-19, the inventors behind the vaccine were not mentioned, with the names invoked being that of pharmaceutical companies. This may indicate a changing of the times, in that science in general has come to rely much less on the individual ‘heroic inventor’ and more on mass bureaucracy.
Rushed Vaccine Approvals
Both vaccinations also had rushed approvals. After the success of the vaccine was announced at a press conference, the FDA approved the vaccine immediately. The Covid vaccines also had extremely short trial periods, but were pushed through under Emergency Use Authorisation under the guise of a ‘pandemic’ in the US and later formally approved.
Mass Participation
One of the key comparisons between these two vaccines was the opportunity for mass participation they provided. This was not just some sort of out there ‘science’ but a real opportunity to participate in the ritual aspects of vaccination practice. There are two key differences: in the Salk vaccine, the mass participation event was the clinical trial, whereas in the Covid case, the mass participation event was the roll out of the vaccine in December 2020. In the Salk case, the participants were children, whereas in the Covid case the participants during the initial furore were adults.
The Salk vaccine had a large number of participants:
Across the United States, 623 972 schoolchildren were injected with vaccine or placebo, and more than a million others participated as “observed” controls.
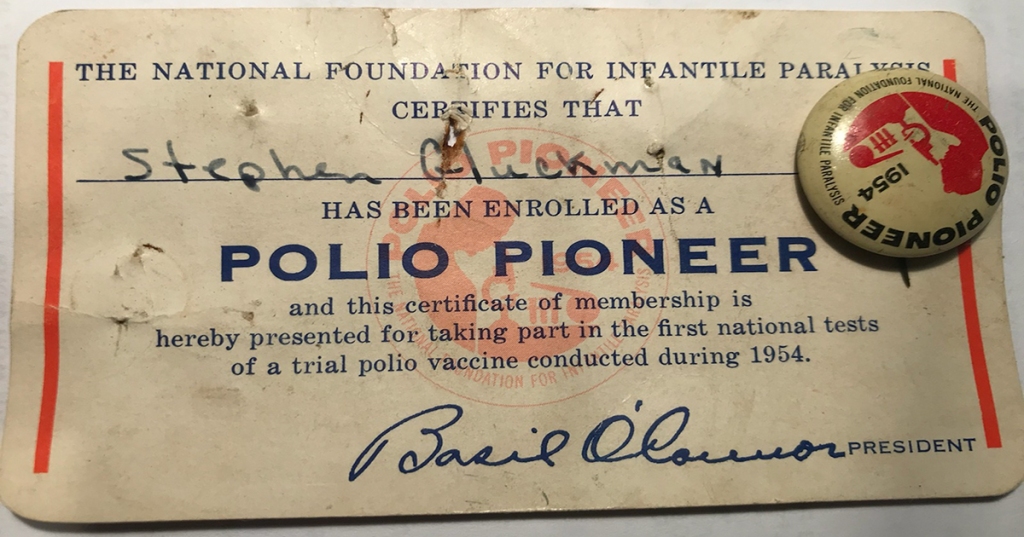
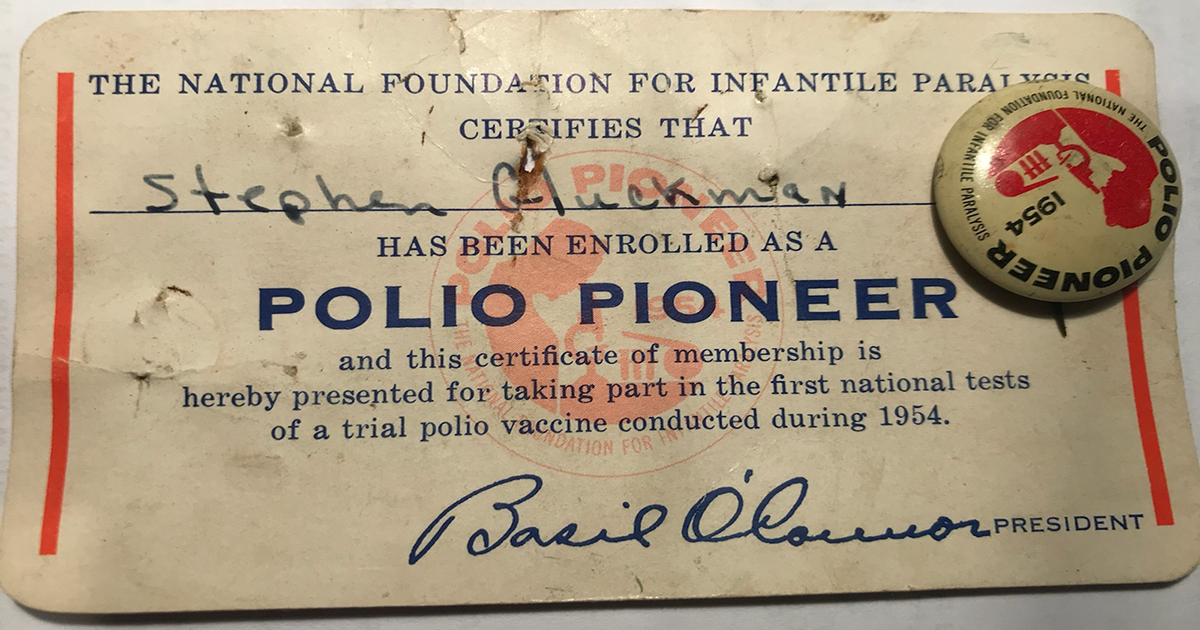
Children were put forward to participate in the trials by their parents, and were called the ‘Polio Pioneers’. They were given badges and certificates as a reward for being injected with the vaccine:
With Covid-19, the mass participation aspect, and the elements of ritualism, came after the clinical trials rather than before. Images were shown of people receiving vaccines, including seemingly gimmicky stories about a man named William Shakespeare receiving a Covid vaccine (complete with imagery).
Because Covid-19 vaccines allowed for adult participation, social media images were used as a means to demonstrate participation in the ritual of vaccination. Ordinary people were given options on platforms like Facebook to put a ‘I’ve had my Covid-19 Vaccine’ banner on their profile as a form of showing that they had taken part in the vaccine ritual.
Both of these strategies for vaccine promotion were dependent on mass technologies that reach the entire country. Mass newspapers, television, and social media were required to sustain this message. But they also required individuals (or their parents) to opt in to this ritual performance on the basis of this propaganda.
In both cases, we see this initial enthusiasm is not maintained. Many people gave up taking Covid vaccines after the first booster, and enthusiasm for the Salk vaccine also waned quickly. Problems such as the Cutter incident, in which the vaccine caused poliomyelitis, caused scepticism. In the US, it was replaced by the Sabin vaccine after this vaccine was field tested in countries like the USSR.
Conclusion
Vaccine campaigns in the 20th and 21st centuries have used mass media as a strategy to create emotional linkage to the idea of taking a vaccine. Encouragement to participate in such events are a means of manipulating the public into vaccination. The idea of ‘being part of’ such a mass project by opting in provides meaning and purpose, and allows the individual to believe that they are playing a part in the banishment of evil.
Smallpox vaccination was said to prevent infection with smallpox. However, there is a significant practical difficulty with this argument, aside from statistical evidence and anecdotes of vaccine failure. This is the nature of ‘vaccine lymph’ itself. Although ‘vaccine lymph’ is often considered to be cowpox, the history is a lot more complicated than this, with multiple different lymph sources in circulation. This poses a theoretical problem for those who argue that vaccination prevented smallpox, since they then have to argue that all these sources are equivalent, but this is unlikely.
Horse Grease Cowpox or Spontaneous Cowpox?
Edward Jenner argued that there was more than one form of cowpox in his essay the Inquiry. His Inquiry starts with a description of a disease of the horse, the grease, which he claims is spread to the cow:
In this Dairy Country a great number of Cows are kept, and the office of milking is performed indiscriminately by Men and Maid Servants. One of the former having been appointed to apply dressings to the heels of a Horse affected with the Grease, and not paying due attention to cleanliness, incautiously bears his part in milking the Cows, with some particles of the infectious matter adhering to his fingers. When this is the case, it commonly happens that a disease is communicated to the Cows, and from the Cows to the Dairy-maids, which spreads through the farm until most of the cattle and domestics feel its unpleasant consequences.
Jenner is clear in this text that the protection comes via the horse, through the cow, to man.
Jenner distinguishes this from spontaneous cowpox, which he considers not protective from smallpox:
It is necessary to observe, that pustulous sores frequently appear spontaneously on the nipples of Cows, and instances have occurred, though very rarely, of the hands of the servants employed in milking being affected with sores in consequence, and even of their feeling an indisposition from absorption. These pustules are of a much milder nature than those which arise from that contagion which constitutes the true Cow Pox. […] But this disease is not be considered as similar in any respect to that of which I am treating, as it is incapable of producing any specific effects on the human Constitution. However, it is of the greatest consequence to point it out here, lest the want of discrimination should occasion an idea of security from the infection of the Small Pox, which might prove delusive.
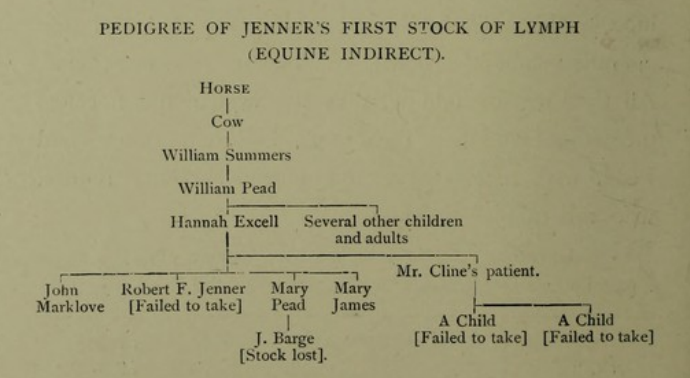
So here we have two forms of cowpox. One protects from smallpox, and one does not. Presumably, the lymph used by Jenner in his vaccinations outlined in the Inquiry was horse grease cowpox.
So where did his next set of lymph come from? Enter William Woodville.
William Woodville was the lead doctor of the Smallpox Hospital in London and interested in Jenner’s method. He was able to obtain lymph for vaccination from a cow in Grey’s Inn Lane, London. Woodville had been previously unable to directly inoculate horse grease on the cow’s teat.
Be it observed, however, that this London cowpox was not Jenner’s cowpox. It was not horsegrease cowpox, but the variety stigmatised by Jenner as spurious.
However, because Jenner had no source of lymph, the Woodville lymph became the source that was spread across the world, regardless of the fact that it wasn’t horse grease cowpox. So if we take the Jennerian distinction as legitimate, there is a significant argument that the lymph used was not protective. Even if we reject the idea that there is such thing as a horse grease cowpox, there is still the problem of which forms of lesions on a cow’s teat are protective from smallpox, since it is agreed that there is more than one form of disease on the cow’s teat.
Cowpox or Smallpox – Was Woodville’s Lymph Contaminated?
As Woodville worked at the Smallpox Hospital in London, he performed his vaccinations there. This of course meant there was a risk of a patient who may become a vaccinifer contracting smallpox, leading to smallpox being spread along with the vaccine lymph. There were also other issues with how Woodville carried out his tests. Although he ran many more tests than Jenner and was more fastidious in recording his results, in some of his cases he performed the variolous test very early on, while the cowpox pustule was still present:
Ann Pink, a tall girl, of a brown sallow complexion, aged fifteen years. This girl was inoculated with variolous matter, on the fifth day, in the same manner as Collingridge, and both tumours proceeded to maturation, though more slowly than in that case.
He then went on to use some of these cases as vaccinifers (e.g. James Crouch was vaccinated, then inoculated on the 5th day after vaccination, then used as the vaccinifer for case 21). This meant the cowpox matter may well be contaminated with smallpox matter.
As Woodville made differing observations from Jenner, regarding the eruptions on the skin, there were some cases where it seemed evident that Woodville’s patients had smallpox.
Horsepox or Cowpox: Equine Lymph Direct From the Horse
Jenner’s relationship to the horse grease theory of cowpox is not straightforward. Essentially, he advocated it initially, but then failed to mention it in his further essays, likely due to its unpopularity. For example, a notable early vaccine promoter, George Pearson, considered the horse grease part of Jenner’s ideas to be nonsense and openly said so. William White argues that Jenner did this for cynical reasons, i.e. financial gain. Later in his life, however, Jenner essentially returned to the horse and in fact used vaccination (equination?) direct rather than via the cow.
For example, he referred to using equine lymph in his correspondence:
[Mr. Melon] sent me some of his equine virus, which I have been using from arm to arm for these two months past without observing the smallest deviation in the progress and appearance of the pustules from those produced by the vaccine.
It was not just Jenner that use horsepox direct. An Italian vaccinator, Sacco, used horsepox to vaccinate.
Sacco obtained some matter from the ulcerous sores on a horse’s hocks (he gives a startling picture of huge, excavated horse sores in his Trattato of 1809), and therewith inoculated several children at the Foundling Hospital of Milan. He found that the effects were very like those of cowpox virus (as we know, in fact, that they always are) ; and, on trying the children with the variolous test, he found that they were protected just as if they had been cowpoxed.
De Carro in Vienna also used horse grease in his vaccinations.
This horse material likely ended up in wide circulation due to its usage by these prolific vaccinators.
Humanised Lymph: Did Serial Passage Affect the Disease?
As for most of the 19th century, vaccination was arm to arm, there is a possibility that passing through multiple human constitutions may have affected the disease. Essentially, this passing through multiple humans was a crude form of serial passage. In fact, people considered this in the nineteenth century as well, which is why some in the 1840s wanted to “return to the cow” and create a fresh stock of lymph (see below). They believed that the passage through multiple human constitutions had made the disease too mild to be effective against smallpox. As virologists subscribe to the idea of serial passage affecting the function of viruses, then they have to concede this is probable in the case of artificial cowpox infection. Thus the vaccine given over time is not a consistent virus but had different mutations, meaning that there is a distinct possibility of mutation away from being an effective preventative of smallpox even if Jenner’s original concoction worked (which of course, it did not).
Cowpox or Smallpox II: Smallpox Via the Cow
In the 1840s, the idea became prevalent that the lymph was no longer potent and that a stock should be raised from cows. The idea that smallpox and cowpox were the same disease became explicit (Jenner had said that horse grease was ‘the source’ of smallpox instead, although he did call cowpox variolae vaccinae i.e. cow smallpox). The reason that cowpox protected from smallpox on this view was that it was smallpox, except passed via the constitution of the cow which somehow made it milder. This idea wasn’t really explained, just asserted.
Cowpox was not a widespread disease, making it difficult to find new lymph sources. As such, there were those who attempted to deliberately infect cows with smallpox to generate these new lymph sources.
One of these men was Robert Ceely, who performed extensive experiments involving cows. He gave detailed descriptions of cowpox and also infected cows with smallpox and described the results.
Badcock was another 1840s writer, who wanted to obtain fresh lymph for vaccination:
The only satisfactory mode of obtaining, with certainty, the true vaccine that presented itself to my mind was, therefore, to inoculate a healthy cow with Small Pox matter, as the result of that operation, if any, must be cow Small Pox
Badcock used this matter for vaccination and indeed states that he vaccinated ‘several thousand’ with this lymph.
Later in the 19th century, when arm to arm vaccination was abandoned, the method of ‘pure glycerinated calf lymph’ came into vogue and emerged as the main method of vaccination. Again, this involved the deliberate infection of cows with smallpox.
The living calf or heifer is first bound down on a movable tilting table, and its belly is shaved and on the clean, tender skin of a most tender part one or two hundred cuts or scratches are then made, and into these cuts or scratches is rubbed some “seed virus,” obtained directly or indirectly from human smallpox.
Vaccinators also tried different examples of less popular material for vaccination.
One example is sheep pox:
Accordingly, when Sacco, in 1804, obtained variolous lymph from infected sheep at Capua, he gave it to Dr. Legni in the remote Sicilian province of Cattolica to try as a substitute for vaccine in the prevention of smallpox.
There were also other examples of various lymph being used – goat pox was experimented with in Madrid in 1804. Crookshank also argued that cattle plague was used for vaccine lymph in India.
The Jennerian Vesicle: The Vaccination Standard
What connects all of this? The notion of the Jennerian vesicle. Basically, the standard for ‘successful vaccination’ was whether it produced a correct ‘Jennerian vesicle’ on the arm where the matter was inserted. In other words, so long as the vesicle looked ‘correct’ the vaccination was considered to be successful. It goes without saying that this is not a scientific criteria for judging immunity to a disease. But because all these sources could raise the Jennerian vesicle, they were defended as vaccine lymph and some were widely employed.
Conclusion
The fact that so many different diseases, from so many different sources, were considered and used as vaccine lymph, poses a theoretical issue for vaccinationists. All these sources were adjudged at some point, and by some individuals to be appropriate matter for vaccination and many sources existed in circulation. Yet it is difficult theoretically to argue that all these sources were equivalent and thus, for the vaccinationist, equally effective against smallpox.
Smallpox vaccination, as practiced for most of the 19th century, was an exercise in filth spreading. It was done via arm to arm vaccination, that is by raising a pustule on one person’s arm and then using that pustule to vaccinate other people in a long chain of vaccinations which went back to an original vaccination with cow pus. This led to a significant spread of disease and vaccine death – that could be covered up by ignoring the source of the disease.
Syphilis
One disease that was spread during the practice of vaccination was syphilis.
It was of course known in the 19th century that syphilis could be spread by sexual activity and could be passed from mother to child (congenital syphilis). Over time, it became more and more obvious that vaccination could also spread syphilis, although this was denied by the authorities for many years.
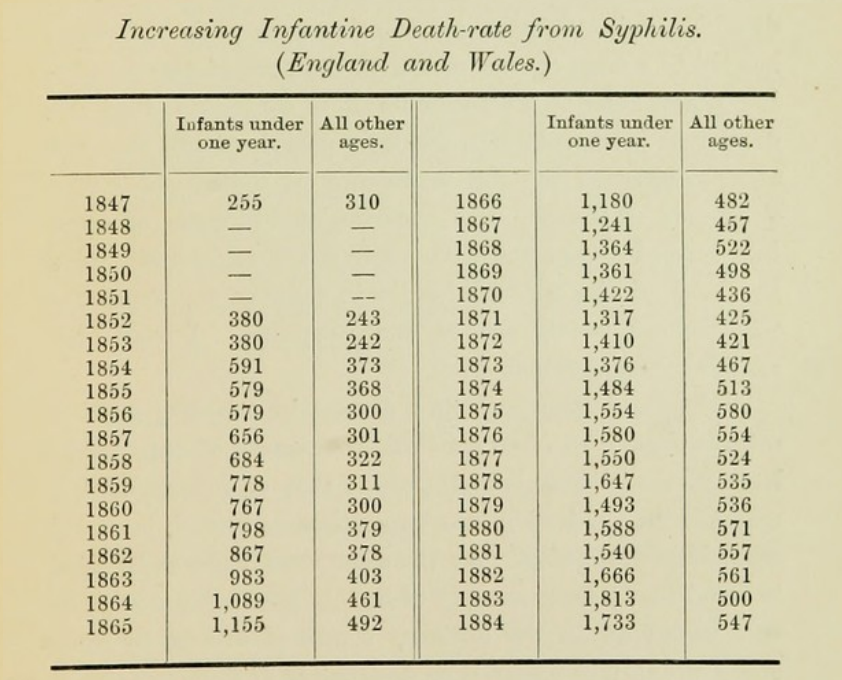
Statistical evidence pointed to the increase in death from syphilis among young children under compulsory vaccination in the United Kingdom. In 1847, before compulsory vaccination, the number of deaths was 255 in England for children under 1 year. By 1884, the number of deaths had increased to 1733. The number shows a steady increase over this time period.
[Table from Creighton’s Cowpox and Vaccinal Syphilis]
There were also several anecdotes that demonstrated the possibility of syphilis after vaccination. P. A. Taylor cites cases where multiple people were given syphilis by vaccination from the same vaccinifer, for example a case where 29 out of 38 children vaccinated contracted syphilis.
Infant syphilis deaths were covered up by blaming the mother’s alleged immorality.
Tuberculosis
Tuberculosis, or consumption, was a common cause of death in the 19th century.
In the UK and Europe, consumption caused widespread public concern during the 19th and early 20th centuries. It was seen as an endemic disease of the urban poor. By 1815 it was the cause of one in four deaths in England. Up from 20% in 17th century London. In Europe, rates of tuberculosis began to rise; in the early 1600s and peaked in the 1800s when it also accounted for nearly 25% of all deaths. Between 1851 and 1910 in England and Wales four million died from consumption. More than one-third of those fatalities were aged 15 to 34; half of those aged 20 to 24, giving Consumption the name the robber of youth.
Anti-vaccinationists suspected that one of the reasons that it was so prominent was vaccination.
In all European armies, vaccination is the order of the day. On their arrival with their corps, the young soldiers are forthwith carefully revaccinated. Now, the military statistics of all countries show an enormous proportion of various forms of tuberculosis among soldiers, especially during the first and second year after their enlistment. […] To sum up, the young soldiers find with their corps material conditions of life, which, for a very large number, are superior to those of their native surroundings. […] Whence then can come these attacks of tuberculosis, so sudden, so numerous, upon subjects that, but a few months before, the council of revision rightly declared to be fit for service.
Some also believed that because cattle can be subject to tuberculosis, the ‘glycerinated calf lymph’ method of extracting vaccine matter (infecting a cow with smallpox and then extracting the matter) might pose a risk.
Leprosy
The spread of leprosy via vaccination was significant mainly in imperial possessions. As colonialism was widespread in the 19th century, one of the items imposed and cajoled onto the native populations was vaccination.
William Tebb describes the situation in Hawaii regarding leprosy. He states that it was completely unknown prior to the introduction of vaccination, but since vaccination was introduced it had spread:
In a leading article on “The Nature of Leprosy” The Lancet, July 30th, 1881, p. 186, says :—” The great Importance of the subject of the nature and mode of extension of leprosy is evident from the steady increase in certain countries into which it has been introduced. In the Sandwich Islands [i.e. Hawaii], for instance, the disease was unknown forty years ago, and now a tenth part of the inhabitants are lepers. In Honolulu, at one time quite free, there are not less than two hundred and fifty cases.”
He goes into detail about how leprosy is spread, showing that while it is not spread by casual contact, it can be spread via inoculation or anything involving piercing the skin. He gives numerous examples of leprosy caused by vaccination and travelled to multiple countries in order to investigate the issue. He found cases not just in Hawaii but also India, South Africa, and other countries. Some cases had the first symptoms at the site of vaccination.
Conclusion
Vaccination was a proven method to spread diseases in the nineteenth century, and in fact, could spread much worse diseases than smallpox (since smallpox either resulted in recovery or death in most cases, whereas these other diseases often led to a slow increase in symptoms). As such the idea that vaccination was a life saver was fatally flawed.
Vaccine deaths have always existed, and have always been denied. This is a story of some of these forgotten vaccine deaths.
Inoculation Deaths
Inoculation, or variolation, was the practice of deliberately infecting someone with smallpox. This was the practice that was used prior to the introduction of the Jennerian method of deliberately infecting people with cowpox as a method to protect from smallpox.
This practice was very dangerous. The more sensible (if that’s the right word) inoculators admitted this risk, they just argued that the odds were better with inoculation than natural infection since they had observed that people generally only got smallpox once.
A man called Jurin (a pro-inoculator) collected statistical data on the question of inoculation. He stated that inoculation had a death rate of 1 in 48 (13 in 624). But that the natural disease killed 1 in 6, so that the odds were better with inoculation (of course, what this logic ignores is that you aren’t guaranteed to get smallpox, and even if you were, you might get it many years later, meaning many life years lost to inoculation).
The Case of John Baker
When Edward Jenner entered into this discussion, he performed experiments on children to attempt to prove that cowpox protected from smallpox. This bit is well known, what is less emphasised, however, is Jenner’s arguments relating to horse grease and cowpox. Jenner believed that there was more than one form of disease of the cow’s teat – horse grease cowpox and spontaneous cowpox. In his initial text, the Inquiry, he argued that the protective form of cowpox was the horse grease form. Jenner believed that the disease was essentially artificial in the cow. The chain of events was as follows, in Jenner’s mind: the horse developed a disease known as grease which affected the heels of the horse. The farrier would have to dress the heels of the horse, causing the disease to be on his hands. However, he also did double duty milking the cow, and as such, then spread the disease to the cow’s teat. Pustules and inflammation developed on the teat as a result and this was horse grease cowpox (which could protect from smallpox).
This is relevant because Jenner wanted to compare direct horse grease with horse grease cowpox. As such, he vaccinated two children, one with horse grease direct and one with cowpox. The child vaccinated with the horse grease was John Baker, a 5-year-old. Jenner had intended to test his immunity by inoculating him for smallpox, but he was ‘rendered unfit for inoculation’, Jenner said, by a fever he caught in the workhouse. The boy died and the most plausible assumption is that he died as a result of the vaccination experiment.
‘Preserving Vaccination From Reproach’
Vaccination death has always been covered up by the medical establishment. As critics of vaccination have pointed out, one way this is done is to put the symptom on the death certificate, but not the cause of the symptom. In this way it can be stated that the child died of erysipelas or some other condition, without blaming vaccination.
What is of interest is we have one case from the 19th century where a doctor openly stated they concealed vaccination as the cause of death on a death certificate. Henry May, a physician from Birmingham (United Kingdom) stated the following in 1874:
A death from Vaccination occurred not long ago in my practice, and although I had not vaccinated the child, yet in my desire to preserve Vaccination from reproach, I omitted all mention of it from my certificate of death.
For much of the twentieth century, deaths from vaccination were higher than deaths from smallpox. Smallpox declined due to increased sanitation:
A Mr. John Cryer, an ardent anti-vaccinationist, taught school in Bradford, Eng. One day he noticed a lad of about twelve years—a new pupil in school. He questioned him: “Where did you come from?” “Sheffield, sir.” “How long have you resided there?” “Six years, sir.” “How many are there in the family ?” “Six of us, sir.” “Then you were in Sheffield during the small-pox epidemic ?” “Yes, sir.” “Did any of you have the small-pox?” “Oh, no, sir, we lived in a front street.” That last sentence tells the whole story. It is worth more than a dozen reports of Local Guardians; worth more than whole columns of statistics. It hits the nail square on the head, and locates the disease. Why didn’t the lad say: “Oh, no, sir, we were all vaccinated?”
Vaccination also declined significantly after the mandates were eased and objection clauses inserted.
Nevertheless we have multiple deaths reported from vaccination. Between 1933-1946 there were 89 child deaths from vaccination according to the official statistics. During the same time 28 died from smallpox. This will likely be a large undercount due to the concealment of vaccination deaths.
This is a very small sample of death that has occurred as a result of smallpox inoculation and vaccination.
The media and governments put a large amount of effort into attempting to manipulate people into taking vaccines, or vaccinating their children. However, these manipulation strategies also exist at the level of the paediatrician. Doctors are armed with strategies that seek to manipulate you into vaccination. Now I would suggest avoiding a doctor’s office as much as possible, but nevertheless we should take a look at the strategies they use to trick people into taking vaccines. Partly to expose the strategy, but also partly to expose how unethical they are.
The CASE approach to ‘vaccine hesitancy’ (as they insist on calling rejection of vaccination) stands for “Corroborate, About me, Science, and Explain/advise.” The analysis of CASE below draws on this linked article to demonstrate the manipulation involved in ‘combating vaccine hesitancy’.
The first thing that we observe is that they need a specific strategy for explaining their case in the first place. I would suggest that this relates quite strongly to the psychology of the physician themselves. As Vaccination is a key Pillar of Faith in allopathic medicine, any challenge to vaccination, no matter how limited, is a threat to the paradigm. I would suggest that one function of having such a strategy is to get the physician to refocus their own thoughts and not get angry at the challenger to the Vaccine Faith (as anger is unlikely to convince anyone to vaccinate).
So let’s explore the strategy. The first aspect of the strategy, Corroborate, is meant to psychologically soothe the patient/parent, by signaling that the concern is acknowledged. This is done by signaling a limited form of acknowledgement of the statement, by stating that they understand where the criticism is coming from. Of course, the doctor won’t do anything such as actually take the concern seriously, no, that would be bad now wouldn’t it. We just have to pretend to humour the anti-vax nutcase so we can get them to jab, jab, jab.
The next step is About Me, that is, explaining how they are so much more knowledgeable on this issue than you. Now, I’m sure as they are always whining about how overworked they are, they have time to read multiple papers about vaccines and much historical discussion of vaccination a week. They completely ignore the fact that many anti vaccine parents have read more literature on vaccines than they have! I would hazard a bet that I have read more literature on vaccines than your average GP and I’m still improving and absorbing information constantly.
Next comes the Science, and by Science here folks we mean repeating information on the NHS/CDC, etc website. Then the explain/advise, which is why the doctor wants you to just take the vaccine already so that they can get more money for their practice. Furthermore, their explain/advise strategy is to try and push you into getting injected immediately, one of the examples given pushes the idea of getting vaccinated ‘today’. I don’t know if anyone’s ever done fraud awareness or the like. One thing you will get told on any fraud awareness webpage is that if anyone tries to rush you into doing something such as handing over details by invoking a sense of urgency that this a red flag for fraud. Now that really sums it all up, doesn’t it?
Image Credit: Photo by Mikhail Nilov on Pexels.com
Currently, the varicella vaccine is not on the UK childhood vaccine schedule, but as of yesterday, the JVCI is seeking to change this.
The Joint Committee on Vaccination and Immunisation (JCVI) has recommended a vaccine against varicella, commonly known as chickenpox, should be added to the UK’s routine childhood immunisation programme.
The vaccine would be offered to all children in 2 doses, at 12 and 18 months of age.
The committee has submitted its recommendations to the Department of Health and Social Care (DHSC), which will take a final decision on whether to implement a programme.
It will probably be rubberstamped, so that they can start giving the vaccine as soon as possible. Of course, we should just ignore the evidence that the JCVI is corrupt and ignored real problems with the Urabe MMR vaccine. Pharma profit is clearly much more important.
The vast majority of people remember getting chickenpox as a child. What happened? You were off school for a week and itched a lot. That was about it. Nothing happened. Your parents weren’t worried. The school wasn’t worried. No one cared. You were possibly told that if you get the chickenpox young, you’re better off. And we need a vaccine for this?
The JVCI has come up with a model to address this problem. Because many people are probably thinking exactly the same as what I’m thinking, even if they support some vaccines. Kind of like when even many Covid fanatics drew the line at injecting mRNA into their five year old because there was no benefit.
The purported justification for this vaccine is some really rare, fringe cases where someone got significantly sick. As such we should inject all healthy children with chickenpox vaccines. Of course this is nuts. The model seeks to play up the risks of chickenpox, and claims that the risks have been underestimated, well of course, what else are they going to say? Now of course we should probably be a bit scpetical given the UK government’s track records with modelling (Neil Ferguson is quite strongly coming to mind at this stage).
The rate of vaccination injury is not even considered in the JVCI model. Even if we assume the vaccine is effective, a very low rate of vaccine injury will massively outweigh any benefits of saving people from chickenpox since well, chickenpox just isn’t very deadly (I can’t believe I have to point this out). Yet the JVCI page online does not mention that adverse reactions as a consideration in their model. Parents having to take a week off work is considered though. Because that is far more important than vaccine injury.
Even more horrible, they want to stick this in MMR, yes, they want to make the MMR vaccine even worse. The only mention of vaccine injury comes in this section with a reference to increased febrile seizures with a combined MMRV vaccine as opposed to MMR + V vaccines. Honestly this rearranging deck chairs on the Titanic while children are poisoned to death. Nevertheless rare, not of concern, etc, standard pro vaccine spiel.
They also seek to justify why they want to promote the vaccine at this time, since, they previously rejected the idea of chickenpox vaccines:
Due to the larger pool of varicella-susceptible children following the pandemic restrictions and, as vaccination is predicted to significantly decrease circulation of varicella, susceptible people may continue to be vulnerable to catching varicella as they head into adulthood.
In other words, let’s use the lockdown that we did to push more of what we want: or, problem-reaction-solution.
They also state that the vaccine recommendation will put us in line with other countries like the United States. Yeah, because we really want to be in line with the United States’ vaccine insanity.
In conclusion, this rather odd sentence from the recommendation stuck out to me:
The community arm of the study estimated the quality adjusted life year (QALY) loss in cases which would not be captured in any medical datasets. This study aimed to assess the impact of mild varicella on quality of life, healthcare use and the financial and health impact on the family unit.
As we can see from the above information, a study was literally done on ‘mild varicella’ i.e. being off school and itching for a week and its effects on ‘quality of life’ and ‘the family unit’. This may seem a bit nuts but trivial, i.e. why would anyone study the effect of being mildly sick for a week? In fact it shows the deeper hubris involved in the vaccination program. All minor inconveniences caused by Nature must be abolished even if it’s being itchy for a week. Consequences? What are those? The idea of a vaccine for everything, no matter how rare or trivial, proves that vaccination is not about our health, but pharma profits and medical hubris.






{kind=link}