One factor often ignored by those analysing autism is the inherent humiliation that is associated with autism. Humiliation is a factor, that unlike other aspects of autism, is worse the intelligence and function of the autistic individual. Intelligence allows the person to perceive their failings, but not to remedy them, resulting in humiliation and shame.
This article will discuss some of the humiliations of autism and why autism essentially means either completely avoiding other people or embarrassing oneself in public on a regular basis.
Sexual Humiliation
In a previous article, I discussed incels and how the incel phenomenon is inherently linked to autism. Autism leads to consistent sexual rejection and frustration.
This aspect of autism involves the obvious, such as attempting sexual approach and inevitability being rejected (because the attempt is always going to show autistic failings, such as poor eye contact, inappropriate comments, etc).
There is also a deeper level to this humiliation. That is the humiliation of never being perceived as sexually desirable and a viable partner. It is beyond the humiliation of an individual rejection.
Nothing can be done about this. Obviously you cannot compel people to find you sexually desirable or want to date you. Thus the only option left is constant burning shame.
Meltdowns
Imagine an adult having a full blown 2 year old style tantrum. That’s what meltdown looks like.
Now imagine having these in public in front of a bunch of people, screaming and crying, etc. Then imagine having to see the people you did this in front of again ever. I have been thrown out of two group therapy groups for doing this, by the way.
Not to mention you have to be aware of this happening at any time. I’ve never done this at work, for example, but it is always a possibility that you could and then get fired.
Which leads us on to…
Unemployment
As explained in previous articles, autistics have an extremely high unemployment rate. Even the intelligent ones. This causes high levels of humiliation as it is embarrassing to never be able to contribute to your family.
Social Incompetence
Not being able to relate to and understand other people also leads to humiliation. This happens when inevitably you say the incorrect thing and everyone else judges you for it. If you are intelligent you always realise after the fact you have said something stupid and then you burn up with humiliation.
Immature Obsessive Interests
Autistic ‘special interests’ are often in childish things, for example obsessing over video games or children’s toys. This again can be embarrassing.
Gait Disturbances
Autism can involve elements of ataxia and poor motor control. For example, I have issues where I still walk on tip toes particularly on my left leg and I have had problems trying to correct this. When I was at school one of my teachers even criticised me for it in drama class. Also there is a high risk of falling flat on your face and tripping over your own feet.
Conclusion
The daily humiliation associated with autism is a factor ignored by all of those in the neurodiversity movement and pro vaccinationists.
This series hopes to explore the history of British Antivaccinationism and Vaccine Scepticism. It is divided into 7 main eras: the period of Inoculation, 1721-1798; the introduction of vaccination, 1798-1853; the imposition of mandates, 1853-1898; the remaining history of the National Antivaccination League, 1898-1972; DTP Vaccine Scepticism 1972-1998; Andrew Wakefield and vaccines cause autism, 1998-2019, and Covid 19, 2020 to present. This section will look at the resistance from ordinary people to vaccination during the late 19th century.
Working Class Antivaccinationism
It had long been pointed out by antivaccinationists that the 1853 mandate was a piece of class legislation. Fines associated with non vaccination were easily payable by wealthy vaccine resistors, but ordinary resistors faced distraint (forced selling of their property) or prison.
Working class antivaccinationists saw vaccination as an attack and a threat to their bodies. They feared a threat to their employment (mandatory vaccination for employment), due to individual cases of employers attempting to force vaccination on their staff, particularly during an outbreak.
Working class people saw vaccination as an assault on their families. During the late nineteenth and early twentieth century, there was a belief among the elite that working class parenting, particularly working class mothering, was inadequate. Working class women were demonised for working (even though economic survival of the family depended on their income) and were seen as failing to contribute good children to a strong British race (see Anna Davin’s Imperialism and Motherhood). Working class people also perceived vaccination as a means of portraying their children as inherently diseased, and thus demonising them as the problem.
Vaccination was also linked to the New Poor Law, which compelled people into the workhouse if they were unable to find sufficient work to survive. The 1840 act which provided free vaccination was done via the Poor Law. Staff who were working in the vaccination program also worked in Poor Law administration. This associated vaccination with pauperism, a connection resented by working class people.
Resistance was associated with the East End of London, as well as certain working class towns, such as Leicester and Gloucester. It was also linked to other working class self improvement movements, such as the temperance movement. Examples of non compliance, other than the obvious refusing to vaccinate, included treating distraint sales as a protest venue, and physical assault against vaccination officers. (For more information about working class antivaccinationism, see the article ‘They Might as Well Brand Us’ by Nadja Durbach).
The largest display of resistance would occur in Leicester in 1885.
The Leicester Protest
Leicester was a hub of vaccination resistance. Antivaccinationist J. T. Biggs gives a very long account of Leicester and how the quarantine methods they employed after the 1871 smallpox outbreak were more successful than vaccination. Most of the city lost faith in vaccination after 1871, and there was a large amount of non-compliance with the vaccination edicts.
In 1885, there was a large protest against the mandatory vaccination laws in Leicester. This protest advocated for individual liberty and rejected the state control of working class children. Mothers stated that they wanted to protect their children from vaccination. The procession down the streets of Leicester included a horse and cow as the representations of vaccine lymph, furniture (as a representation of the distraint sales mentioned above) and an effigy of Edward Jenner. Further meetings also took place after the protest, stating the continued intent to resist vaccination.
Conclusion
Today, antivaccinationism is often portrayed by vaccinationists as a ‘privileged’ position advocated for by primarily middle-class mothers. If we look at history we can see this is far from the case and that many ordinary people were committed antivacciantionists.
Both neurodiversity activists and those who consider autism to be negative but also promote vaccination consider a 1 in 30 autism rate to be normal for humanity. 1 in 30 is the approximate current rate of autism among children in the United States. As these groups believe that autism is genetic, it must follow that they consider this rate to be relatively consistent across recorded history, because the human genome has not radically changed over this period. As such, it follows that, even given the limitations of recorded history in terms of preservation of evidence, there must be significant evidence of autism in past societies.
In this post, I am simply employing informed common sense to the idea that, for example, the Roman empire or Victorian London had a 1 in 30 autism rate.
It is surprising, when you look at their posts and accounts, how little plausible evidence they are able to dredge up of autism examples prior to the twentieth century. I don’t rule out a few cases of autism existing before vaccines because it is possible that substances such as aluminium, mercury, etc could have got into someone’s brain in another way. Usually, neurodiversity activists point to say, Isaac Newton, or some other example of a figure considered to be positive in history as an example (funnily enough, I have never seen them point to someone who is considered to have had a negative impact on society).
But to prove autism is normal, a few scattered examples are not enough. They have to prove 1 in 30, or they at least have to prove close enough that 1 in 30 is a plausible extrapolation. At this, they have failed miserably. In fact, I haven’t even seen an example where they make the attempt.
Another significant problem for the account that autism is natural is the unemployment rate and financial burdens of autism and its relation to human societies. We can use an employment rate as a reasonable proxy for the ability to function in a society. In the United Kingdom, the unemployment rate for autism is 78%. If we do a little simplification on the maths, we can use two-thirds unemployment as a rate generous to autism. Then, if we simplify our 1 in 30 rate to 1 in 33 or 3/100 to give us a rough approximation, it follows that if 3/100 people in the population are autistic and 2/3 of those cannot work due to autism, then 2/100 of the population is unemployed due to autism.
Think about this for a moment. Really think about it. Does it seem plausible that societies with fewer modern economic resources could sustain such a population? No.
We can start by going back within the past 50-125 years with modern welfare state systems. Are we supposed to believe that governments never noticed the huge amount of benefits being spent on autistic children and adults? Especially more conservative governments, who are always talking about the need to cut benefits? While estimates of the economic burden of autism are necessarily rough and somewhat problematic, it has been stated that to provide for an autistic without intellectual disability costs around a million pounds when taking into account all economic costs.
Going back further, in the Victorian era, there were systems such as Poor Law relief and as a last resort workhouses. Are we supposed to believe that no one noticed severely autistic children as a cause of this burden on families?
If we want to go back further, do we really believe that hunter-gatherer societies could have dealt with such an autism rate? Even high functioning autistic people would have been a heavy burden because of the necessity for communication and social cohesion in these societies.
As such, autism promoters need to provide some hard proof that this autism rate is normal and natural before I am even willing to consider that vaccines are not the primary cause.
Think about what the CDC’s grotesque vaccine schedule does to the relationship between parents and their children. The kid does not know what’s going on. Yet every few months the parents offer up the child to strangers who inflict pain with sharp metal objects while smiling, laughing, and saying “it’s okay,” “you’re a champ.” The shots can cause fever, digestive problems, seizures, and worse for days, months, or even years. The parents go through this Molochian ritual over fifty times. The child has no words to express what’s happening. The child cannot possibly give consent. The psychological scars from this betrayal are permanent and the child learns to never trust the parents again.
Parents teach the idea of not following herd mentality. How many times have parents said “If so and so jumped off a cliff, would you?” to their children? How about this – if the white-coat told you to push your own child off the cliff, would you do it? Of course the answer is no, it’s only yes if the cliff is disguised as a sterile lighthouse shining light across the sea of disease. But nevertheless – if the white-coat told you, would you do it? Everyone is aware of the Milgram experiment. Vaccination is society’s Milgram experiment writ large, so insidious the authority of the white-coat that parents will destroy their own children.
Let’s see how this goes. A parent takes their child to be vaccinated, seeks the white-coat for the ‘well baby check-up’. Or perhaps not, perhaps the parent has some doubts about the shots, but the authority of the white-coat’s fanaticism removes this well enough. The child – probably in discomfort, fear, receives the holy baptism of the injection. However when they get home they aren’t right. They are having seizures, or a fever (dosed with paracetamol/acetaminophen no doubt, which aggravates the injuries). Then everything gets worse. The child stops speaking, stops making eye contact, loses skills. The white-coat gaslights the parent and claims the child was always this way, always damaged. The parent knows this is a lie, as there is nothing wrong with their memory.
The parent seeks those in the same boat with them, and the few doctors who will not lie to them about their children’s injury. They speak out about the child being vaccine-injured. They unite with other parents to tell the truth about vaccines. They promote and amplify doctors and experts telling the truth about vaccines. So far there is no problem: the gaslighting establishment medics need to be exposed as liars and frauds. Parents can give powerful testimony to the way their children were destroyed by vaccines.
So where is the problem?
The reality of the vaccine-injury movement – with the exception of the Covid ‘vaccine’, and to a lesser extent the Gardasil vaccine – is that the vast majority of those speaking are parents. This certainly applies very strongly to specifically autistic vaccine-injury. In part this is out of necessity: some autistic people are simply too severely vaccine-damaged to communicate regarding their injuries. In part this is out of the success of the ‘neurodiversity’ movement that convinces those with ‘high functioning’ autism that autism makes them special and unique and that there is nothing wrong with it. Nevertheless this necessity creates a skew, that those with are personally autistic vaccine-injured don’t get a voice or a prominent role in the vaccine-injury movement.
You can try this for yourself: when you think of people speaking about autism and vaccine injury, who first comes to mind? When I test this on myself, I come up with Robert F Kennedy, Jr, Andy Wakefield, JB Handley, Jenny McCarthy, Christopher Exley, Del Bigtree, you get the idea. No autistic people whatsoever. This creates a problem. Parents can articulate what they observe their child do and the distress of their child from the outside. Any medical professionals can describe what they have seen in injured children. Journalists can accurately describe the corruption. Doctors and journalists and advocates but no-one of any profile is doing this from the inside.
But now we must trespass on even more controversial territory, that is the question of guilt.
Does anyone else know what a paradox it is? That I can appreciate parents who speak out about their child’s vaccine injuries while feeling such bitterness and anger? To know that your parents love you but that they also ruined you for life?
And then this brings us to the most fundamental question: who is ruined? We can do this in a very simple way. Let’s use an example. Andy Wakefield has talked in interviews about the children in his 1998 Lancet study and how the parents of the vaccine-injured children were told that they should stick their child in a home, because ‘that’s autism’ and nothing could be done to help them. What is unsaid that – well fundamentally, that’s true. Not in the sense that nothing could be done to ease the child’s suffering, necessarily – but in the sense that the parent has the full capability to abandon their vaccine-injured child and walk away, whereas the child has no such luxury to abandon their vaccine-injuries. Don’t misunderstand me: I am not saying that this would be easy to do or would cause no distress to the parent. Just that it is possible: and therein lies the problem. The parent is intact: distressed, angry, feeling guilt, but nevertheless intact.
Parents of vaccine-injured children need to unconditionally be defended from the gaslighting mainstream medical establishment. I am happy to put my bitterness and anger aside for The Cause. After all, nothing matters more than making sure that there are no more human beings like me. But I will never be silent, and if there is a certain amount of discomfort in that refusal, then that is how it will have to be.
Since the 1990s, the idea of ‘neurodiversity’ has become a cottage industry. The basic tenet of neurodiversity is that autism is a perfectly normal variation of human development that should not be seen as a negative trait. It seeks to highlight the alleged ‘positive’ traits of autism and believes that the struggles of people with autism are largely caused by society not being accepting rather than the inherent downsides of the condition. This article will seek to discuss three parts of this phenomenon by comparing two theories of autism: the neurodiversity theory of autism and the iatrogenic theory of autism i.e. vaccine injury. The first part will discuss the evidence for each theory, concluding that vaccine injury has a large amount of evidence to support it. The second part of this article will look at the individuals and institutions that promote each theory and how the media portrays each group. The third part will draw it together by explaining how the neurodiversity theory is constructed as an alternative to deflect from the vaccine injury theory and to gaslight people suffering with autistic vaccine-injury and their parents about their experiences.
This is part II of the three part series.
Part II: Two Narratives
Having made the case that vaccine-injury is an extremely plausible theory of autism, I will now examine the contrast between how advocates of the neurodiversity narrative and advocates of the vaccine-injury narrative have been treated by the establishment. Although the neurodiversity narrative claims to be countercultural and in opposition to the ordinary view of autism, in reality it is promoted by mainstream sources. On the other hand, vaccine-injury theorists – including those who have backed their theories up by significant evidence – have faced consequences from being smeared to the loss of their career.
Is Neurodiversity Countercultural?
The neurodiversity narrative claims to be countercultural. As it is a fairly recent narrative, it portrays itself as the up and coming new narrative to ‘reframe’ autism in a positive light. In fact, the article I quoted from in Part I makes this argument, comparing it to different theories of autism:
The mainstream perspective – the perspective that autism is caused by a genetic defect and should be cured by targeting the autism gene(s).
The fringe theory – the theory that autism is caused by environmental factors like vaccines and pollution and should be cured through addressing these factors.
This narrative takes aspects of the ‘social justice’ style narrative, where those that are marginalised by society are reframing themselves as positive actors, reframing what is considered as ‘negative’ by society as a positive.
Of course, there is a long history of narratives claiming to be counterculture, when in fact, they are nothing of the sort. A good example, that has some similarities with the neurodiversity ideology, is transgenderism. Transgender ideology claims that opposite sex impersonators are a marginalized group, whereas in reality those who oppose them are censored, sacked, and smeared. Men playacting as women are promoted, celebrated and glorified in the media, with any criticism deemed as bigotry. Pharmaceutical companies support this narrative for profit, and many sinister actors use it is as a means of promoting transhumanism.
So is the neurodiversity narrative really countercultural?
In general, the best way to check if a narrative is against the establishment is to look at what the establishment actually says about it. If the establishment contains a large amount of institutions promoting a particular narrative, and is spending a lot of money on promoting a particular narrative, then there is a reason for that. So let us examine what the interconnected establishment/media/NGO complex actually states about autism and neurodiversity. This will look at several different groups: autism charities, the media, the fiction industry and other significant actors.
Autism Charities and Consultancy
Although some people would like to consider charities to be not ‘establishment’ institutions, in reality large charities are part of the establishment. Their role in society is to advance narratives that benefit establishment interests, but while seeming as if they are independent advocacy groups.
To give an example already alluded to in Part I, the Alzheimer’s Society expresses some scepticism that aluminium accumulation in the brain is the cause of Alzheimer’s disease. To acknowledge this would be bad for the establishment, since it is (elite) human action that unleashed aluminium on the environment and caused high levels of exposure. Questioning aluminium exposure in this case might lead one to come to the conclusion that the establishment does not have a concern for human health. Furthermore, obscuring the reality in this case allows Big Pharma to sell expensive patented drugs for Alzheimer’s disease, rather than reducing exposure or reducing aluminium in the human body. Foreign policy is another area where charities can be demonstrated to serve elite agendas. For example, human rights organisations will focus on violations of, say, freedom of speech by ‘enemy countries’ such as Russia, while ignoring the same or worse by Western countries or allies such as Saudi Arabia.
Of course, the issue is even more explosive when it comes to questioning vaccines, since vaccination is essentially the cult of the modern age:
Vaccinating everyone on earth (the goal of the Gates Foundation, W.H.O., Pharma, and presidents of both political parties) has nothing to do with health; its sole function is to give atheists in the developed world a feeling of heroism that supplies them with a sense of symbolic immortality.
There is no known ‘cure’ for autism. We also believe that autism does not need a ‘cure’ and should be seen as a difference, not a disadvantage. We also warn people about fake cures and potentially harmful interventions here.
This does not mean that autistic people do not face challenges, but with the right support in place, they are more than capable of living fulfilling and happy lives.
This is, of course, the neurodiversity narrative. On the other hand they say that vaccines don’t cause autism, because that idea must be opposed at all costs.
It is also worth noting that there is an entire industry of autism ‘consultancy’, which is designed to promote neurodiversity, particularly relating to employment. There are a whole bunch of services available, for example, Aspire Autism Consultancy provides “bespoke neurodiversity training for therapists and healthcare practitioners.”
It is also worth noting that if you do want accommodations at work related to autism as a disability, you are basically obliged to put up with the neurodiversity framing.
The Media
The mainstream media is another crucial plank of the establishment, that serves their interests. The purpose of the media is not to present the news in an objective way, but to be propaganda for the powers that be. The structure of the mainstream media goes through multiple filters and each one excludes any opposition voices to ensure a conformity of thought.
There are plenty of articles in the media promoting the neurodiversity agenda. A survey of the media carried out by pro neurodiversity activists found the following result (abstract only available):
Results showed increased coverage of neurodiversity and neurodivergent individuals from 2016 to 2022. Key findings include an increase in calls for representation, advocacy, and the recognition of neurodiversity as a different neurotype rather than a condition to be cured.
Recently in the UK, there has been a programme hosted by Chris Packham, and autistic man and advocate for neurodiversity about autism and ADHD (ADHD is also considered to be an example of neurodiversity by advocates, and is also possibly vaccination injury although, unlike autism there is not as much evidence to prove this). I haven’t watched the programme because I don’t want to waste the energy getting angry about the obvious misrepresentation of autism that will exist within the program. It is worth noting that the programme about autism was nominated for a television award, meaning that it must have been viewed as in line with what the media and establishment wish to promote. Articles in the media have also promoted this programme, and called it moving (even the more right leaning Telegraph, which is, say, more sceptical of similar ideologies like transgenderism).
The Fiction Industry
Fiction may seem as if it is separate from the establishment, but in reality the establishment has a significant influence here as well, particularly when it comes to television. For example, it is a well-known fact that a large number of American movies are produced with the help of the intelligence agencies.
If there are characters, action or dialogue that the DOD doesn’t approve of then the film-maker has to make changes to accommodate the military’s demands. If they refuse then the Pentagon packs up its toys and goes home. To obtain full cooperation the producers have to sign contracts, called Production Assistance Agreements, which lock them into using a military-approved version of the script. [emphasis in original text]
So how are autistic people portrayed in the media? There is but one model of the autistic film or TV character and that is the ‘autistic savant’. That is, someone who is socially inept but a genius at doing some weird obscure thing which wins the character the things that they want in life. In some portrayals a biting satirical wit might be added, particularly in comedy programs, with an edge of intellectual superiority played for laughs. Sheldon Cooper of The Big Bang Theory is the best example of this.
This is basically the neurodiversity model in action. Look at those special characters that think differently that have all these wonderful things like a PhD and an amazing job! No-one puts low functioning children who have to use a diaper and are non-verbal on the TV. No-one puts the 6′ 2″ 30-year-old man with a mental age of 5 who flies into incandescent, violent rages over sensory triggers on the TV. Why would they? So fiction gives an extremely misleading picture of autism to the public that bolsters the neurodiversity model.
Although neurodiversity advocates might also complain about the portrayal of autism in the media, the reality is that it is only their own ideology being reflected back at them. The special, unique one who ‘thinks differently’: that is their argument of what autism is, not mine, and that is their portrayal of what autism is, not mine.
Conclusion
As we can see from the above collection of evidence, the establishment has expressed a significant amount of support for neurodiversity.
The Vaccine Injury Approach to Autism and Its Critics
Vaccine-injury advocates have been treated rather differently by the establishment. This section will discuss a few different advocates of the autism-vaccination link: Dr. Andrew Wakefield, Dr. Christopher Exley, and Jenny McCarthy.
Dr. Wakefield Redux
The most obvious place to start on this topic is the demonisation of the British gastroenterologist, Dr. Andrew Wakefield. Dr. Wakefield is infamous among the vaccine pushers, and his name is invoked like that of the devil himself. Dr. Wakefield has been the subject of a thousand lies by the mainstream media and medical establishment. Eventually, he was struck off the medical register in 2010. His career was destroyed. So what was his ‘crime’? Simply to take parents seriously when they observed their children regressing into autistic behavior after the MMR vaccination.
So let’s look at how Dr. Wakefield got interested in the issue of the MMR vaccine and autism. After Dr. Wakefield performed studies on measles and gut issues, specifically Crohn’s disease, he was contacted by parents who saw their child regress into autistic vaccine-injury after their MMR vaccination. Dr. Wakefield and his colleagues at the Royal Free Hospital in the UK produced a case series of 12 of these children called, “Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children” published in the Lancet in 1998. Contra claims made by the mainstream media, which is to this day constitutionally incapable of representing this paper accurately, it was not designed to ‘prove’ that the MMR vaccine causes autism. The people who made the initial link between the MMR and autism were the parents of those children, not Dr. Wakefield.
Onset of behavioural symptoms was associated, by the parents, with measles, mumps, and rubella vaccination in eight of the 12 children, with measles infection in one child, and otitis media [ear infection] in another.
This eventually led to him being relentlessly attacked by Brian Deer, a Telegraph ‘journalist’ who was obsessed with destroying his career. Deer made multiple false claims about Dr. Wakefield and his study. These false claims included the claim that Wakefield and his colleagues did not have ethical approval for the medical testing that they ran on the ‘Lancet 12’ children and that Dr. Wakefield misrepresented the case histories of those children to push a narrative blaming the MMR vaccine. Deer also claimed that Wakefield had unethical conflicts of interest. As a result of these claims, Dr. Wakefield was eventually struck off the medical register in 2010. There is much more detail to this story not able to be discussed here for space considerations, so I suggest reading this article by Iain Davis if you would like a refresher on the full picture.
[Wakefield] is the sacrificial lamb and a stark warning to any scientist, medical practitioner or researcher who dares to challenge the corporate dictatorship. The MSM’s annihilation of Dr. Wakefield served two purposes. Firstly to convince a misinformed public that any who suggest vaccines may not all be wonder drugs are ‘evil’ and also to put the fear of God into the scientific community.
IAIN DAVIS – ‘THE EVISCERATION OF DR. ANDREW WAKEFIELD’
Dr. Christopher Exley
Dr. Christopher Exley is former Professor of Bioinorganic Chemistry at Keele University in the UK. He did his Ph.D. on aluminium exposure among fish and the harm that this can cause and is an extremely credible expert on the interaction of the neurotoxin aluminium with human and animal life. As shown above, he has studied the link between aluminium and autism (and other diseases such as Alzheimer’s disease and Multiple Sclerosis). He led the Aluminium Research Group and published around 200 papers on aluminium.
So what happened to Dr. Exley after he published his group’s paper on ‘Aluminium in Brain Tissue in Autism’?
The first thing to note is that the media has attacked Dr. Exley. The Guardian accused him of pushing ‘anti-vaccine misinformation’:
A British academic who has promoted anti-vaccine misinformation has raised more than £150,000 through a university donations portal to support his research during the coronavirus crisis, the Guardian can reveal.
They quote a vaccine promoter stating that Dr. Exley’s paper is ‘bad science’ but of course do not elucidate the audience about why it is bad science (the reader doesn’t need to know that, they just need to know which hate figure ‘anti-vaxxer’ of the week they need to condemn).
Prof Chris Exley angered health experts for claiming that tiny amounts of aluminium in inactivated vaccines, such as the HPV and whooping cough inoculations, may cause “the more severe and disabling form of autism”.
They, of course, did this in order to try to make sure that the funding portals were shut down so the research could not continue (not that Keele needed any encouragement on this front – see below).
The case of Dr. Exley also reveals something else important about our media – the principle that experts are only experts until they question vaccination, then they become ‘misinformation’. Dr. Exley was an acceptable expert for the Guardian to cite when it came to the Camelford poisoning. This case involved aluminium was accidentally dunked into residents’ drinking water in Camelford in Cornwall. One woman, Carole Cross, died from a rare form of Alzheimer’s after this poisoning, with extremely high levels of aluminium in her brain. Dr. Exley is acting within his expertise by commenting on both cases, but only one is considered to be acceptable.
Keele University basically made Dr. Exley’s position at the university untenable for questioning the safety of aluminium adjuvants in vaccination.
Since that time [about 2015], the university has progressed from spiking Exley’s press releases and downplaying or ignoring major scientific contributions by Exley’s research group to — perhaps most concerningly — sabotaging the research donations that are the “lifeblood” of independent-minded scientists.
On the 11th of April 2019, following receipt of a number of emails from potential donors unable to make a donation using the online link, I was told by someone called Lee Bestwick in Finance that he had been instructed to disable the donations portal set up by Finance on my behalf. He was not aware that there had been no prior discussion with me about this.
We appreciate your interest in the University and in our research staff who are undertaking such a wide range of interesting and pioneering work, but hope you understand the delicate balance we must maintain to ensure our public and private reputation.
Kennedy wrote in response:
I must consider that your decision to return my personal check is likely the product of the pharmaceutical industry’s open, aggressive, and rather sinister campaign to defund Professor Exley. Vaccine makers view Dr. Exley’s efforts to accurately characterize, for the first time, the health impacts of aluminum adjuvants in vaccines, as a threat to their profit-taking. Terminating Professor Exley’s research has been a central objective of the $50 billion vaccine industry. This cartel wants the world to believe that aluminum in vaccines is safe despite the lack of any safety studies to indicate that is possible, and plenty of peer-reviewed literature that suggests that it is not.
[A] recent letter to Exley from Keele University’s dean of natural sciences explained that “the university will no longer provide facilities to solicit or enable restricted charitable donations” to support the Exley group’s research on “the bioinorganic chemistry of aluminium and its links to neurodegenerative disease.”
The dean clarified that this would include “donations from individuals, groups, charities and foundations” — amounting to the entirety of the group’s research income.
Eventually due to this disruption of funding the research group was shut down despite having around 200 peer reviewed publications.
Furthermore, Dr. Exley was suggesting methods by which to detox from aluminium and remove it from the body in order to reduce autistic symptoms. The method Dr. Exley suggested was drinking mineral waters with a high silicic acid content, as silicic acid binds to aluminium and then it is expelled from the body via urine. Again Dr. Exley demonstrated this through science, showing increased excretion of aluminium after consuming a litre of silica water. When done on a consistent basis (daily) this reduces the body burden of aluminium including in the brain and improvements in symptoms are observed (Dr. Exley witnessed this in Alzheimer’s disease). Not only was he showing what had harmed us, he was helping us with his protocol, and I can vouch that it works personally because I have tried it.
So now we can see that Dr. Wakefield is not the only person to lose his career for questioning the links between vaccines and autism.
Jenny McCarthy: Demonised Mothers
Jenny McCarthy is a media figure who spoke out about the safety of vaccination after her son, Evan, regressed into autism after receiving the MMR vaccine. McCarthy is different from the cases I have highlighted above in that she is the mother of a vaccine injured child. Her role as a mother affects her portrayal by the vaccine industry.
Generally speaking, mothers are considered less competent observers of their children than doctors, despite the fact that the doctor only sees the child for brief appointments and the mother is around the child 24/7. This is justified by the medical establishment, because they consider themselves to be the ‘experts’.
There is a significant amount of misogyny in the portrayal of McCarthy in the media. For example, news articles often introduce her as ‘former Playboy model Jenny McCarthy’ or other similar framing when talking about her scepticism of vaccination. The fact that McCarthy was involved in the pornography industry has no obvious relevant connection to her scepticism of vaccines. Except, in the mind of the vaccinationist, it is clearly related, since they always mention it.
The purpose of this framing is to invoke the Madonna-Whore complex, a misogynistic trope in which women are always the idealised, perfect mother, or the debased whore. Because McCarthy posed for Playboy, the implication is that she is inherently an unfit mother, unqualified to observe her son’s regression into autism. The other implication is that she is inherently stupid (women who have worked in pornography are perceived in society as ‘dumb bimbos’). Thus she is unable to correctly observe the behaviours of her own child in the mind of the vaccinationist.
Conclusion
Neurodiversity cannot be seen as an anti-establishment narrative. Like transgenderism, it is an ideology promoted by the establishment that pretends not to be promoted as such. In part III, we will discuss the target of the neurodiversity narrative – high functioning autistic people and parents of autistic children – and how this precludes vaccination criticism.
This series hopes to explore the history of British Antivaccinationism and Vaccine Scepticism. It is divided into 7 main eras: the period of Inoculation, 1721-1798; the introduction of vaccination, 1798-1853; the imposition of mandates, 1853-1902; the remaining history of the National Antivaccination League, 1902-1972; DTP Vaccine Scepticism 1972-1998; Andrew Wakefield and vaccines cause autism, 1998-2019, and Covid 19, 2020 to present. This section forms part 2 looking at Jenner and his critics.
The ‘Discovery’ of Edward Jenner
In 1796, Edward Jenner performed his first vaccination. This was on an 8 year old boy called James Phipps. In this experiment, Jenner inserted into the arm of the boy matter from the teat of a cow with cowpox using a lancet. Cowpox was a disease of the cow’s udder, which caused pustules to appear on that area. It was transmitted to humans via the action of milking a diseased udder.
Jenner’s justification for doing this was that cowpox allegedly prevented smallpox. There had long been a rumour among dairy maids that they could not contract smallpox, if they had contracted cowpox. In fact, the official story or mythology of Edward Jenner states that he overheard this idea from a dairy maid when he was a teenager and was taken with testing it (this is narrated by Jenner’s sycophantic biographer, John Baron).
Jenner became a country doctor in Berkeley, Gloucestershire. He became a member of the Royal Society after writing a paper about cuckoos that was accepted. In 1796, when Jenner performed his first inoculation with vaccine virus (later known as vaccination) he wrote a paper outlining his theory of the origins of cowpox (he believed that it originally came from the horse, and was transferred to the cow via those who dressed diseased horse heels). He then outlined the theory that the cowpox infection prevented the smallpox infection. He used some examples of those he met in his practice who had had a cowpox infection, on whom inoculation (deliberate infection with smallpox) would not ‘take’. The failure of inoculation to take was interpreted as immunity to smallpox. He also outlined his test on James Phipps, first inserting cowpox matter and several weeks later performing inoculation on the boy. As the inoculation did not take Jenner interpreted this as proof of immunity.
The Royal Society rejected Jenner’s paper. They believed it did not have enough evidence to support it and that it might tarnish Jenner’s reputation. Jenner was still determined to publish, so he added more evidence – increasing the number of cases of vaccination. (A detailed discussion of the differences between Jenner’s first and second versions of the paper can be found in Crookshank’s book). He published it in 1798.
Pearson and Woodville
Two important figures took up Jenner’s vaccination idea, George Pearson and William Woodville. Both these doctors were vital in spreading the practise of vaccination and backing it ideologically.
William Woodville was the lead doctor at the Smallpox Hospital in London, so it can be imagined that he had significant influence over the treatment and prevention of smallpox. He took to the idea of vaccination and ran a significant number of tests. Woodville’s tests had many flaws, in particular that he sometimes attempted cowpox and smallpox inoculation very close together. However his testing was more extensive and better documented than Jenner’s.
Pearson sought to set up an institute for vaccination. This annoyed Jenner, as he was not consulted in advance regarding the project. Pearson also distributed vaccine lymph early on in the process to allow other doctors to perform vaccination, which was important as Jenner did not have vaccine lymph to give out on many occasions.
Jenner had a significant number of supporters in the medical profession. When he was put forward for a government reward in 1802, a large number of doctors spoke in his favour. The profession adopted Jenner’s theory very quickly, and it spread widely. This included across Europe, the United States, as well as many colonised countries.
Jenner’s Critics
Jenner had three main critics of his theory when it was first published. These three men were Benjamin Moseley, John Birch, and William Rowley. None of these men were antivaccination in the sense that we would understand this term today, i.e. they were not opposed to all artificial inculcating of disease. They were supporters of the old method of inoculation and sceptical of Jenner’s attempt to replace it. At this time, there were no high profile critics of both inoculation and vaccination (this tendency would only develop post vaccination mandate, from 1853).
These three men opposed the award to Jenner by the British government during the hearing on this issue in 1802.
Benjamin Moseley
Moseley was a doctor who was well known for other writings prior to his involvement in the vaccination controversy, in particular writings relating to the Caribbean.
He opposed Jenner’s method early on, and published more than one book relating to the issue. He considered that a ‘cowpox mania’ had taken over the medical profession. In his book, A Treatise on the Luis Bovilla, Or Cow Pox, he made several arguments. He stated there was no affinity between cowpox and smallpox, so there was no specific property of cowpox which meant it could prevent smallpox. He also argued that cowpox was not necessarily a mild disease. He pointed to the ulceration that often accompanied the practise.
John Birch
John Birch was a surgeon who was opposed to vaccination. In his text, Serious Reasons for objecting to the Practice of Vaccination he discusses the Royal Commitee on Vaccination. He argued that there was a large number of vaccine failures but that most of these were not admitted, and that the Committee tried to soften the language by stating that these cases only apparently had cowpox.
William Rowley
William Rowley was an active practitioner of inoculation. As such it could be said that he had a degree of vested interest in defending the practise against the new threat of vaccination. He considered inoculation to be a very safe practise that rarely led to death when performed competently. Vaccination, on the other hand, he considered both dangerous and ineffective.
Rowley authored a work called ‘Cow Pox No Security Against Smallpox Infection‘. This book has been considered a target of mockery by vaccinationists due to a couple of the images included in the book. These images claimed to show vaccination injuries, but as Rowley had titled one of them ‘The Ox Faced Boy’ he was mocked for making a linkage between vaccination and people becoming bovine.
Rowley actually collected a large number of cases, including with address details so at the time they could be checked, of vaccination injury, death, and cases of smallpox after vaccination.
He also provides an extensive list of excuses used by vaccinationists to defend their theory. These included the theory of ‘spurious cowpox’, which was outlined by Jenner in his second essay on cowpox. The idea of a ‘real’ and a ‘spurious’ cowpox allowed any cases of failure to be assigned to a spurious vaccination. He also accused vaccinationists of misdiagnosis of cases of smallpox in vaccinated people. He also states that vaccinationists formulated the excuse that even if cowpox failed to prevent the disease, it made it milder.
Conclusion
Vaccination had some significant opposition. However, it is fair to say that it had very little ideological opposition at this time. Its opponents thought it was unsafe and ineffective but advocated the earlier practise of inoculation instead rather than rejecting both. Well founded ideological opposition to vaccination would have to wait until after 1853 – the year of the UK’s smallpox vaccine mandate.
This series hopes to explore the history of British Antivaccinationism and Vaccine Scepticism. It is divided into 7 main eras: the period of Inoculation, 1721-1798; the introduction of vaccination, 1798-1853; the imposition of mandates, 1853-1902; the remaining history of the National Antivaccination League, 1902-1972; DTP Vaccine Scepticism 1972-1998; Andrew Wakefield and vaccines cause autism, 1998-2019, and Covid 19, 2020 to present. This section forms part 1, looking at the inoculators and their critics.
The History of Inoculation
Inoculation was the practise of deliberately infecting someone with smallpox. The theory behind the practise was that a person could only get smallpox once, and would then get what we would call natural immunity. Although this concept was not understood, it was observed that smallpox was only contracted once. As such, by selecting the time and place of infection, and by carrying out additional practices such as the following of certain diets, smallpox could be rendered a milder disease with a greater chance of survival.
Lady Mary Wortley Montagu observed the practise of inoculation in Turkey and had one of her children inoculated while over there. She introduced the practise to her physician, Charles Maitland, who was taken with the idea and began to practise inoculation on willing members of the elite. There was a brief fad for this practise initially, but the first wave of enthusiasm died out quite quickly, and the number of inoculations performed was still very small. Some doctors tried to collect scientific data relaying to inoculation, such as Jurin, who attempted to figure out the death rate from inoculation versus the death rate from natural smallpox infection – he calculated it at about one in 50 for inoculation versus 1 in 6 for the natural disease. On this basis, he argued for the supremacy of inoculation but acknowledged that it had some risk.
Inoculation became more widely practised later on in the 18th century and particularly in the second half of that century, with the rise of the Suttonian method of inoculation, which was less harsh on the body. Daniel Sutton was able to widely promote his method among elites, and inoculation became more popular. The Suttonian method was that in practise before it was replaced by the cowpoxing method associated with Edward Jenner.
The Masseys – The Original Anti Vaccinationists
In response to the introduction of inoculation, two men, Isaac and Edward Massey, brought objections to the table against the new practise. They could be considered the original antivaccinationists. Each of the Masseys put forward a different approach to the issue.
Edmund Massey’s religious objections
Edmund Massey was a Christian clergyman at a church in London, and he objected to inoculation on religious grounds. He preached a notable sermon in 1722 against the new practise which was distributed in written format. The first argument he uses against inoculation is that it is forbidden for man to deliberately inflict disease. He states that while the Bible furnishes examples of men healing when given divine power, there are no examples of men directly inflicting disease. Instead, God inflicts disease to test people’s faith and to punish sin. He raised the book of Job as an example of this.
Isaac Massey’s scientific objections
Isaac Massey raised scientific objections to inoculation. He was an apocethary (which was quite vaguely defined but involved working in the medical profession). In his book, A Short and Plain Account of Inoculation, he raised several different scientific objections to the practise. For example, he claimed that those who were inoculated were not necessarily getting genuine smallpox. He pointed out that it was an uncertain procedure, despite the claims of the inoculators to the contrary that factors such as age and the time of year can be controlled.
He stated that inoculation was ‘a disease of their own making and procurement’. He argued that when true smallpox is spread by inoculation, it can also spread to other people, such as in the case of the inoculation of Mary Batt, which spread smallpox and led to the death of a servant. He argued for living a sober lifestyle as a means to reduce the risk from smallpox.
In his book addressing Jurin’s statistical claims, he argues that Jurin did not allow for factors such as age, disease and poverty when calculating comparative death rates. Most who would have been inoculated when Massey was writing would have been elites, who would have had a better rate of survival from natural smallpox due to more adequate nutrition and being less likely to live in complete squalor. He thus considered that Jurin was not comparing like with like. He also pointed out that inoculation may spread other diseases. He pointed out that the initial claims of the inoculators was that the procedure was harmlessly and that this had to be revised when deaths occurred.
Conclusion
The objections to inoculation did not prevent the practise from eventually becoming widespread in certain elite circles. Inoculation formed the ideological basis for Jenner’s much more well known vaccination practise.
Since the 1990s, the idea of ‘neurodiversity’ has become a cottage industry. The basic tenet of neurodiversity is that autism is a perfectly normal variation of human development that should not be seen as a negative trait. It seeks to highlight the alleged ‘positive’ traits of autism and believes that the struggles of people with autism are largely caused by society not being accepting rather than the inherent downsides of the condition. This article will seek to discuss three parts of this phenomenon by comparing two theories of autism: the neurodiversity theory of autism and the iatrogenic theory of autism i.e. vaccine injury. The first part will discuss the evidence for each theory, concluding that vaccine injury has a large amount of evidence to support it. The second part of this article will look at the individuals and institutions that promote each theory and how the media portrays each group. The third part will draw it together by explaining how the neurodiversity theory is constructed as an alternative to deflect from the vaccine injury theory and to gaslight people suffering with autistic vaccine-injury and their parents about their experiences.
Part I: Two Theories
There are two main theories of autism. The first theory states that autism is genetic, and the second theory states that autism is iatrogenic. The first theory is advocated by both people who think that autism is a good thing, and by those who think it is a bad thing. The latter group of people, who believe that autism is a net negative but who also believe it is genetic, will not be discussed in this article. Instead we will be comparing the ‘autism is a positive, genetic gift’ group (the ‘neurodiversity’ group) to the ‘autism is iatrogenic, largely caused by vaccination’ group (the ‘vaccine-injury theory’ group). Part I will outline these two theories and look at the evidence.
The Neurodiversity Theory of Autism
What is the ‘neurodiversity’ theory of autism? It can be summed up by saying that autism is not a disability, it is a difference that should be celebrated. If you search for ‘neurodiversity’ you can find all sorts of articles advocating for this. Here’s one picked at random:
Neurodiversity is a movement that wants to change the way we think about autism. It rejects the idea that autism is a disorder and sees it instead as a neurological difference: one with a unique way of thinking and experiencing the world.
The movement focuses on celebrating neurological diversity and championing the different world-views and skills that autistic, dyslexic, bipolar, and other neurodiverse people have.
The idea of ‘neurodiversity’ has been increasing in popularity as a paradigm to ‘explain’ autism.
Of course, saying that autism is a positive trait does not explain it. So neurodiversity theorists use genetics to explain autism.
I will argue that both sides of the neurodiversity coin are false: having autism is always a negative thing, and that genetics does not explain autism.
Let’s start with the genetics aspect. One significant piece of evidence that the autism-is-genetic advocates use is twin studies:
Since the first autism twin study in 1977, several teams have compared autism rates in twins and shown that autism is highly heritable. When one identical twin has autism, there is about an 80 percent chance that the other twin has it too. The corresponding rate for fraternal twins is around 40 percent.
On the surface, twin studies look like exceedingly convincing evidence. They have been used to argue for a genetic link for a varying range of problems, including schizophrenia. In reality, though, twin studies are not good evidence that autism is genetic.
The problem that we run into is that twins are likely to have had the same environmental exposure, and this is doubly true when it comes to vaccination. No parent is going to vaccinate one of their twins and not vaccinate the other in some sort of science experiment. Thus both twins will be getting very similar exposure to aluminium, thimerosal, etc. via vaccinations. (Though see this caveat: aluminium levels in vaccination can vary significantly when vials are actually examined). The other major issue with twin studies is that they conclude that interaction between the body and these kinds of exposures is ‘genetic’. A genetic propensity to, say, accumulate certain toxins may well exist in autism cases. But in order for autism to develop, exposure to the toxin is required, and exposure to a toxin is not genetic. The same weakness applies when looking at alleged genes that have been associated with autism – it could be that those genes simply predispose a person to toxin accumulation.
The main weakness in the genetic case for autism is below:
It goes without saying that human genes have not radically changed since 1970. So how can the autism rates have changed so drastically? Autism-is-genetic advocates have tried their best to explain this graph, but they have done a bad job of it, because the whole graph screams ‘environmental causes’. But let’s have a look at their explanations for an increase in autism.
The main explanation offered is that the definition of autism has got wider and that is why these numbers have increased so much. Intuitively, this is a really poor explanation, for a number of reasons. For a start, we are looking a massive, massive increase. 1 in 10,000 to 1 in 30 is huge. To explain this simply by stating ‘it’s increased diagnosis’ is intuitively and logically implausible. People who argue this, I think, don’t understand how large a proportion of the population 3% is. That is a very significant chunk of the population. Older people here can employ their common sense. Were 3% or more of your childhood colleagues autistic? If you doubt that you could tell, I assure you that you can with just a little thought. Poor eye contact is a dead giveaway for autism, as is just an obvious awkwardness. The reality is, even ‘high functioning’ autistic people just seem odd, weird and off in particular ways so I would say you could almost always tell. Furthermore, the unemployment rate for people with autism, according to UK government data, is 78%. If we approximate the data, if 1 in 30 people are autistic and 2/3 (being generous) cannot work, this means around 2% of the population cannot work due to autism. The idea that government institutions never noticed 2% of the population being unemployable due to autism is laughably implausible.
This hypothesis also does not fit the shape of the graph very well. It keeps curving upwards, rather than seeing a bump for a change in diagnostic criteria and a levelling. The graph has still not levelled off. At some point, you have to start asking questions.
This issue also becomes more difficult to cover up when you consider severe autism. Autistic people who have a basic level of functioning in the ‘real world’ may just come across to normal people as a bit weird. In these people’s case, it’s more possible that they may not have a diagnosis. This would not be the case with those with severe autistic deficits. Again this is another argument that is just absurd on the face of it:
You can’t have missed 97 percent of the children in the ’80s who had autism. They’re trying to get the public to believe that kids who spin in circles, don’t speak, don’t socialize, can’t go to the bathroom by themselves all existed in our public high schools and elementary schools in the ’80s but only today have gotten a proper diagnosis. It’s incomprehensible.
Aside from being intuitively implausible, one study on this issue concluded:
In summary, the incidence of autism rose 7- to 8-fold in California from the early 1990s through the present. Quantitative analysis of the changes in diagnostic criteria, the inclusion of milder cases, and an earlier age at diagnosis during this period suggests that these factors probably contribute 2.2-, 1.56-, and 1.24-fold increases in autism, respectively, and hence cannot fully explain the magnitude of the rise in autism.
But what about the claim that autism is always a net negative? Surely that’s a little bit fundamentalist? After all, some of the advocates of the neurodiversity theory are autistic themselves, right, and surely they would know? So let’s tackle this thorny question.
The most obvious piece of evidence to start with is life expectancy. The evidence demonstrates that autism significantly decreases life expectancy. This is pretty mainstream evidence that can be found with a quick search.
One study, published in the American Journal of Public Health in April 2017, finds the life expectancy in the United States of those with ASD to be 36 years old as compared to 72 years old for the general population.
In other words, according to this study autism halves life expectancy.
The other study was published by the British Journal of Psychiatry in January 2018. This was a Swedish study showing similar results but elaborating on other causes of death as well. This study showed a life expectancy in those with ASD with a cognitive disability (or a learning disability) at 39.5 years versus 70 years for the general population studied. Those with ASD without a learning disability had an average age of death at about 58 years.
Furthermore, most of these causes of death are inherent to autism. For example, being much more likely to die in an accident. Autistic people have poor motor control and are much more likely to have these kinds of accidents such as drowning that lead to death. Horrific anxiety at normal experiences, such as sensory issues around normal noise/light/smell stimuli, also increases mortality as the body becomes overwhelmed with the constant anxiety triggers, meaning that the body’s ability to fight cancers is impaired, and heart attack and stroke risk is increased. People with autism are also unemployed/unemployable, with only about 20% of autistic people even being employed in the UK. This is linked to having awful social skills, having severe anxiety, and in some cases being completely non verbal and non functional. Being perennially unemployable is bad for your health; higher unemployment rates have been well established to be linked to mortality in sociology.
A study that followed autistic people for 20 years showed even more negative outcomes, although most of the participants also had other intellectual disabilities.
The outcome data was grim, showing pervasive inability to live independently, hold a job, or manage money. Few became independent, with 99% unable to live independently. Of those, 70% lived at home with relatives, 21% lived in disability homes in the community, and 8% in residential facilities. A mere 3.7% attained postsecondary education, about half of those representing certificates from college disability programs. While the majority were considered incapable of holding a job in the competitive workspace, some worked in disability workshops or other sheltered positions. Most participants were incapable of handling money, even with caretaker assistance, with only 9.5% considered capable.
The neurodiversity paradigm likes to attempt to escape from this reality by claiming that this is purely down to ‘society’ refusing to accept us. That argument is nonsense. The argument is most obviously flawed when it comes to those with severe autism, since any range of accommodations will not fix deficits such as being non verbal, not being able to go to the toilet by yourself, seizures (comorbid with autism), extremely poor motor control, severe gastroenterological issues (linked to autism), sensory issues and meltdowns, etc. If a neurodiversity advocate would like to explain how ‘acceptance’ will fix these problems, the comment section is all theirs. But it is even pretty much nonsense when it comes to ‘high functioning’ autism as well. The reality is ‘acceptance’ and accommodations only really make a difference in edge cases when it comes to solving the issues outlined above. Take for example ability to work. The severely impaired autistic person will never be able to work, you can throw all the accommodations in the world at the issue, it’s not going to happen. Whereas, a high functioning or borderline high functioning autistic person may be able to work if given a few accommodations. I’m not arguing against accommodations. What I am arguing against is the idea that accommodations, or society being more accepting of autism will fix our problems. It won’t.
As for the supposed ‘positive’ aspects of autism, what are they? Usually, it is claimed that many people with autism are more intelligent and analytical than normal people. However, this is likely to confuse correlation and causation. The most plausible explanation here is that brain development is more likely to be disrupted by toxins in the case of intelligent people due to more dense neuron growth in highly intelligent people. And again, severe cases of autism are erased by this view. It glorifies a very narrow spectrum of individuals with autistic injury – the ‘autistic savant’ – while writing off the harms done to the rest.
So what about the people with autism diagnoses who make the claim that autism is a positive thing and that neurodiversity is valid? Well, if someone with an autism diagnosis saying something settles the question, then autism is a devastating vaccine-injury that destroys and obscures the true personality of the individual, rather than reflecting it. Because of course this author has an autism diagnosis. So this kind of argument gets us nowhere.
The Vaccine-Injury Theory of Autism
There is an alternative, ‘underground’ theory of autism which advocates for the view that autism is (at least primarily) caused by vaccination. This article will discuss one cause of autism that the author believes has been comprehensively documented, that is aluminium adjuvants in vaccination entering the brain, disrupting the housekeeping cells of the brain (glia and microglia)and triggering inflammatory reactions such as the il-6 pathway. This is not to say that there are no other problems with vaccination as it relates to autism or no other possible causes (e.g. thimerosal). This article will stick to one cause for reasons of length and clarity.
I will go into a little bit more detail on the basic theory, before discussing the evidence. Aluminium is used in ~80% of vaccines as an adjuvant (substance used to promote an immune response). It is in the vast majority of childhood vaccines, excluding the MMR. However, aluminium is also a neurotoxin that the body cannot filter out effectively when injected, and because of this it can enter the brain. In short, the mechanism of how the injury occurs is like this. The aluminium in a vaccine is injected into the body. Immune cells are stimulated to respond to the site of injection. These immune cells (macrophages) respond and ‘swallow’ the aluminium. But when any inflammatory event in the brain occurs, these cells will be called upon to help, but instead will bring a massive payload of toxic aluminium with them into the brain.
A set of nine criteria used to determine the strength of an association between a disease and its supposed causative agent. They form the basis of modern medical and dental epidemiological research.
The more of the Bradford-Hill criteria you can demonstrate, the more likely it is that A causes B. Let’s look at these criteria with relevance to the fact that vaccines cause autism.
The first factor we can discuss is coherence. In other words, “does the association fit with other facts?” In the case of the above theory, it fits very well with facts about aluminium.
Aluminium is toxic to the human body. Aluminium has no biological function in human life and so its presence in the human body is always a net negative. The idea than aluminium, at least, can be toxic is widely accepted. Furthermore, it is accepted that aluminium can enter into brain tissue. Even more than this, it is accepted that it can cause harm once it gets into the brain tissue. One form of aluminium toxicity where this occurs has been observed in dialysis patients:
[A]luminium toxicity occurs due to contamination of dialysis solutions, and treatment of the patients with aluminium-containing phosphate binding gels. Aluminium has been shown to be the major contributor to the dialysis encephalopathy [“damage or disease that affects the brain”] syndrome and an osteomalacic component of dialysis osteodystrophy.
In stating this so far, I haven’t deviated from accepted science. Slightly more controversial than this is the idea that Alzheimer’s is caused by aluminium in the brain. This idea has been around since 1965 according to the Alzheimer’s Society. Although some people doubt the correlation-causation relationship (I would argue more for financial reasons than scientific), there is evidence from a wide range of sources.
The Scotsman reported on a study performed by researchers looking at aluminium levels in drinking water that found people in areas with higher levels of aluminium were more likely to die of dementia. The study’s author said:
We still see this well accepted finding that higher levels of aluminium in particular are associated with an increased risk of dementia. It’s confirmatory rather than anything else. [my emphasis]
Dr. Chris Exley has done multiple studies showing high levels of aluminium in the brains of those who died with a diagnosis of Alzheimer’s disease.
Animal studies also provide further evidence for the fact that aluminium in injurious to the brain. Dr. Christopher Exley observed, when he was studying fish, that when the fish were exposed to aluminium, they would start hanging out in the corner of the tank. Another study, performed by a sheep farmer (and shown in the Bert Ehgartner documentary, Under the Skin), showed that sheep injected with aluminium adjuvant (even without an antigen) showed much higher levels of aggressive behaviour and did things like grind their teeth on metal railings. Mice are also negatively affected by aluminium:
Male mice in the “high Al” group showed significant changes in light–dark box tests and in various measures of behaviour in an open field. Female mice showed significant changes in the light–dark box at both doses, but no significant changes in open field behaviours.
Thus, aluminium was clearly affecting the neurochemistry of the animals, and these behaviours are decent proxies for autistic symptoms in humans (aggression being analogous to autistic meltdowns and the fish acting strangely being analogous to social avoidance).
All of this evidence is a strong case that the aluminium factor in autism is coherent. We know aluminium is toxic and can harm the brain. Therefore that it can cause the kind of behavioural issues that we observe in autism cannot be prima facie ruled out. This is Criteria 1 on our Bradford Hill list solidly met.
The next criteria we can discuss is dose-response relationship. In short, if we give more aluminium adjuvants to children, do we see an increase in autism? Recall our graph from above – the 1-in-10000 to the 1-in-36 increase in autism prevalence. Now let’s compare this to the increase in aluminium adjuvants and thus exposure.
Shaw and Tomljenovic wrote a paper addressing this topic:
By applying Hill’s criteria for establishing causality between exposure and outcome we investigated whether exposure to Al from vaccines could be contributing to the rise in ASD prevalence in the Western world. Our results show that: (i) children from countries with the highest ASD prevalence appear to have the highest exposure to Al from vaccines; (ii) the increase in exposure to Al adjuvants significantly correlates with the increase in ASD prevalence in the United States observed over the last two decades (Pearson r=0.92, p<0.0001); and (iii) a significant correlation exists between the amounts of Al administered to preschool children and the current prevalence of ASD in seven Western countries, particularly at 3-4 months of age (Pearson r=0.89-0.94, p=0.0018-0.0248).
The correlation here is strong – more doses, more autism. The dose-response relationship is in this data. Point 2 on the Bradford Hill Criteria list is met.
The third factor that we can discuss is strength of association. Or in other words, how much is the difference in observed rates of autism between the vaccinated and the unvaccinated? This question is not all that easy to answer, mostly because information on this kind of question has been suppressed.
Dr. Paul Thomas has revealing evidence on this question.
Dr. Paul Thomas is the most successful doctor in the world at preventing autism. Data from his practice show:
If zero vaccines, autism rate = 1 in 715;
If alternative vaccine schedule, autism rate = 1 in 440;
If CDC vaccine schedule, autism rate = 1 in 36.
[…]His alternative vaccine schedule reduces autism risk by more than 1200%. However even an alternative vaccine schedule increases autism risk by 160% versus no vaccines at all.
The difference between 1 in 715 and 1 in 36 is huge. This is evidence of a significant strength of association between two factors. Of course the historical evidence showing fewer cases of autism among older people and more among the young with a strong correlation also matches up with this evidence, since older people are comparatively ‘unvaccinated’. So that’s our third criteria met.
The fourth factor we can discuss is temporal relationship. In other words, the effect must follow, not precede exposure. This factor is difficult to elucidate with vaccines, because exposure is so early on in life, including in the first day of life in the US. This is used by the vaccine cult to argue for the genetic position, but also ensures that it is more difficult to prove that exposure causes the symptoms because the exposure is so early and rampant. However, the simple observation of vaccines preceding autism is almost always true (unless the child is unvaccinated) because if you expose the child at day 1 (US) or 2 months (UK) that is before autistic behaviour is observed. So in a way, their rampant pushing of vaccinations has met this criteria all by itself.
We also haveanecdotal evidencefor this factor, that is, parents observing their child regressing into autism after vaccination. Of course, anecdotal evidence is automatically dismissed by any Pharma apologist. It is true that when using anecdotal evidence, there are significant pitfalls to consider. People can misremember things, or actively lie. These points are worthy of consideration.
However, both of these risks are minimised in the case of assessing autistic regression after vaccination. In terms of lying, there is simply no motive for a parent to lie about observation of regression into autism after a vaccine. Suggesting to a paediatrician, for example, that a child’s autism was caused by a vaccine will lead to being attacked and dismissed by the doctor. Parents are also attacked in the media if they suggest this idea, such as in the case of Jenny McCarthy, who has been subject to hit pieces because she stated that the MMR vaccine caused her son’s autism. Although vaccine advocates state that parents are likely to fall for the idea that someone is to blame for their child’s autism (such as doctors or Pharma) this is also unlikely. The parents had to consent for the vaccine to be given, and so you would expect to observe the opposite: parents denying that vaccines cause autism, since then they would have to blame themselves for consenting to the vaccine(s) and human beings do not like to acknowledge guilt.
Being mistaken about observation is also less likely in the case of autistic regression. This is because we are talking about parental observation of children and decent parents are highly alert to any signs of illness in a child, particularly a child of the age likely to receive vaccines. I will concede however that it is not impossible for someone to either be mistaken or lie. However it is quite implausible that given the factors weighing against these that all cases are examples of lying or misremembering given the multitude of testimonies that we have.
Thus there is at least some evidence for criteria four on the Bradford-Hill list.
The fifth factor that we can discuss is consistency. In other words, if we introduce aluminium adjuvants to all sorts of different groups, rich, poor, black, white, Asian, male, female, etc, do we see increased levels of autism?
There is a male-female disparity in autism diagnosis, with males being significantly more likely to be diagnosed than females. There is likely some biological reason why boys are more susceptible to this form of aluminium poisoning that is currently unknown (or at least, unknown to me). Nevertheless we see an increase in autism diagnosis in both groups.
The sixth factor we can discuss is experimental evidence. In other words, do we have any hard evidence for aluminium in the brain in autism? The answer to this is yes.
Dr. Exley and his research team examined this question directly. They obtained samples of brain tissue from individuals that had died with a diagnosis of autism. This was the first study of this kind. They examined this brain tissue and found very high levels of aluminium in all samples.
The aluminium content of brain tissue in autism was consistently high. The mean (standard deviation) aluminium content across all 5 individuals for each lobe were 3.82(5.42), 2.30(2.00), 2.79(4.05) and 3.82(5.17) μg/g dry wt. for the occipital, frontal, temporal and parietal lobes respectively. These are some of the highest values for aluminium in human brain tissue yet recorded and one has to question why, for example, the aluminium content of the occipital lobe of a 15 year old boy would be 8.74 (11.59) μg/g dry wt.?
We can add another one of Exley’s papers to make this evidence even better. This paper by Exley and Clarkson contains control samples who died with no signs of neurodegenerative disease:
The aluminium content of each lobe (mean and SD) were 1.03 (1.64), 1.02 (1.27), 0.95 (0.88), 0.77 (0.92) and 0.51 (0.51) μg/g dry wt.
These samples have much lower levels of aluminium in them than the autism samples, and this is despite the fact that the controls were mostly older than the autism samples – meaning lifelong exposure to aluminium through non-vaccine routes would have been higher and it would have had more time to accumulate in the control tissues.
The main limitation of this evidence as pointed out by its critics is that the study had a small sample size of N=5 when it came to measuring aluminium concentration in the autism samples (and for some aspects of the study N=10). This was for practical reasons (i.e. there isn’t a large amount of samples of autistic brain tissue available).
It is fair to acknowledge this, and obviously it would be better if the sample size was larger. However, it is completely dishonest to dismiss this study because of the small sample size. This study, for example, is completely different from a survey where 5 participants answering would be worthless. We are looking at pathological brains with clear evidence of a high level of a neurotoxin in them. The level of neurotoxin in these brains cannot be explained away by saying that there is only a few of them. To have that level of brain aluminium content and for it to not be pathological and negatively affecting the cells around it is absurd, unless you want to straight up deny that aluminium is neurotoxic.
Furthermore, no-one has tried to either confirm or reject the Aluminium Research Group’s findings (to this author’s knowledge at least). The establishment haven’t done a study where they demonstrate that the levels of aluminium found by the group are overly high. This is another case where the establishment claim the evidence isn’t good enough to support an anti-establishment view and then just ignore the question. So, despite establishment criticisms, this is criteria six on our Bradford-Hill list met.
We can use Exley’s evidence to discuss the seventh criteria, biological plausibility.
The 2018 paper shows that the high levels of aluminium were found associated with glia and microglia:
Discrete deposits of aluminium approximately 1 μm in diameter were clearly visible in both round and amoeboid glial cell bodies (e.g. Fig. 3b). Intracellular aluminium was identified in likely neurones and glia-like cells and often in the vicinity of or co-localised with lipofuscin (Fig. 5). Aluminium-selective fluorescence microscopy was successful in identifying aluminium in extracellular and intracellular locations in neurones and non-neuronal cells and across all brain tissues studied (Fig. 1, Fig. 2, Fig. 3, Fig. 4, Fig. 5).
This is important because those cells are disrupted in autism. For example, they are responsible for synaptic pruning, which does not occur correctly in autism.
Aluminium-loaded mononuclear white blood cells, probably lymphocytes, were identified in the meninges and possibly in the process of entering brain tissue from the lymphatic system (Fig. 1).
The eighth criteria we can discuss is specificity. The idea of specificity ideally means that one disease has one cause, but this is difficult to apply to reality as Bradford Hill acknowledged. Aluminium adjuvants, in reality, are highly likely to cause more than one disease. However, the argument is not just that aluminium adjuvants cause autism, but that a specific action of aluminium adjuvants causes autism. Our theory offers a specific toxicant (aluminium), a specific route of exposure (injection), a specific method by which that toxin gets into the brain (macrophages), specific cells that are disrupted (glia and microglia), and specific negative cascades that are triggered (excessive IL-6 production due to an inflammatory response). Our argument also does not claim that glial disruption by aluminium adjuvants causes a whole host of problems, but autism specifically (and nothing else). So the theory meets criteria eight on the list.
The last factor we can discuss is analogy. If we can observe similar things happening that makes our own theory more likely to be true. This is easy to demonstrate in the case of aluminium poisoning, as poisoning by different metals, such as mercury, can cause significant impairments in child functioning. One interesting case worthy of discussion here is that of acrodynia. Acrodynia, or ‘Pink disease’ was an early 20th century disease that symptomatically had some overlap with autism although with some differences. It was later proven that pink disease was a form of mercury poisoning caused by mercury teething powders. We know from this case that metal poisoning can cause symptoms with some similarities to autism. There are also examples of aluminium itself causing other forms of poisoning, which were discussed in point 1. So analogy also supports our case and gives us point 9.
Conclusion
As we can see from the above discussion, the idea that vaccines cause autism is strongly evidenced. However, the theory is also opposed by the entire establishment despite this evidence. It is to how these two differing theories of autism are treated that we now turn.
Smallpox vaccination, as practiced for most of the 19th century, was an exercise in filth spreading. It was done via arm to arm vaccination, that is by raising a pustule on one person’s arm and then using that pustule to vaccinate other people in a long chain of vaccinations which went back to an original vaccination with cow pus. This led to a significant spread of disease and vaccine death – that could be covered up by ignoring the source of the disease.
Syphilis
One disease that was spread during the practice of vaccination was syphilis.
It was of course known in the 19th century that syphilis could be spread by sexual activity and could be passed from mother to child (congenital syphilis). Over time, it became more and more obvious that vaccination could also spread syphilis, although this was denied by the authorities for many years.
Statistical evidence pointed to the increase in death from syphilis among young children under compulsory vaccination in the United Kingdom. In 1847, before compulsory vaccination, the number of deaths was 255 in England for children under 1 year. By 1884, the number of deaths had increased to 1733. The number shows a steady increase over this time period.
[Table from Creighton’s Cowpox and Vaccinal Syphilis]
There were also several anecdotes that demonstrated the possibility of syphilis after vaccination. P. A. Taylor cites cases where multiple people were given syphilis by vaccination from the same vaccinifer, for example a case where 29 out of 38 children vaccinated contracted syphilis.
Infant syphilis deaths were covered up by blaming the mother’s alleged immorality.
Tuberculosis
Tuberculosis, or consumption, was a common cause of death in the 19th century.
In the UK and Europe, consumption caused widespread public concern during the 19th and early 20th centuries. It was seen as an endemic disease of the urban poor. By 1815 it was the cause of one in four deaths in England. Up from 20% in 17th century London. In Europe, rates of tuberculosis began to rise; in the early 1600s and peaked in the 1800s when it also accounted for nearly 25% of all deaths. Between 1851 and 1910 in England and Wales four million died from consumption. More than one-third of those fatalities were aged 15 to 34; half of those aged 20 to 24, giving Consumption the name the robber of youth.
Anti-vaccinationists suspected that one of the reasons that it was so prominent was vaccination.
In all European armies, vaccination is the order of the day. On their arrival with their corps, the young soldiers are forthwith carefully revaccinated. Now, the military statistics of all countries show an enormous proportion of various forms of tuberculosis among soldiers, especially during the first and second year after their enlistment. […] To sum up, the young soldiers find with their corps material conditions of life, which, for a very large number, are superior to those of their native surroundings. […] Whence then can come these attacks of tuberculosis, so sudden, so numerous, upon subjects that, but a few months before, the council of revision rightly declared to be fit for service.
Some also believed that because cattle can be subject to tuberculosis, the ‘glycerinated calf lymph’ method of extracting vaccine matter (infecting a cow with smallpox and then extracting the matter) might pose a risk.
Leprosy
The spread of leprosy via vaccination was significant mainly in imperial possessions. As colonialism was widespread in the 19th century, one of the items imposed and cajoled onto the native populations was vaccination.
William Tebb describes the situation in Hawaii regarding leprosy. He states that it was completely unknown prior to the introduction of vaccination, but since vaccination was introduced it had spread:
In a leading article on “The Nature of Leprosy” The Lancet, July 30th, 1881, p. 186, says :—” The great Importance of the subject of the nature and mode of extension of leprosy is evident from the steady increase in certain countries into which it has been introduced. In the Sandwich Islands [i.e. Hawaii], for instance, the disease was unknown forty years ago, and now a tenth part of the inhabitants are lepers. In Honolulu, at one time quite free, there are not less than two hundred and fifty cases.”
He goes into detail about how leprosy is spread, showing that while it is not spread by casual contact, it can be spread via inoculation or anything involving piercing the skin. He gives numerous examples of leprosy caused by vaccination and travelled to multiple countries in order to investigate the issue. He found cases not just in Hawaii but also India, South Africa, and other countries. Some cases had the first symptoms at the site of vaccination.
Conclusion
Vaccination was a proven method to spread diseases in the nineteenth century, and in fact, could spread much worse diseases than smallpox (since smallpox either resulted in recovery or death in most cases, whereas these other diseases often led to a slow increase in symptoms). As such the idea that vaccination was a life saver was fatally flawed.

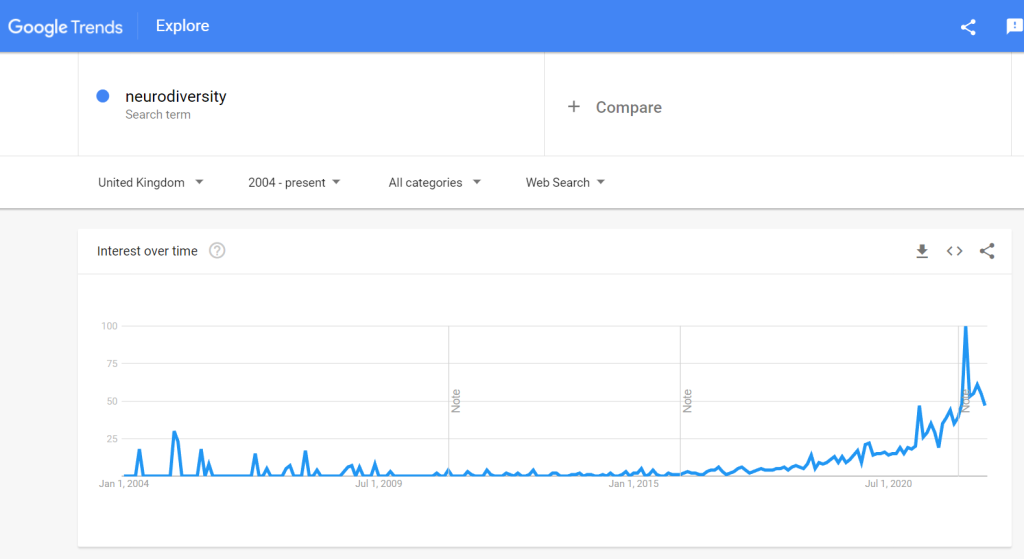
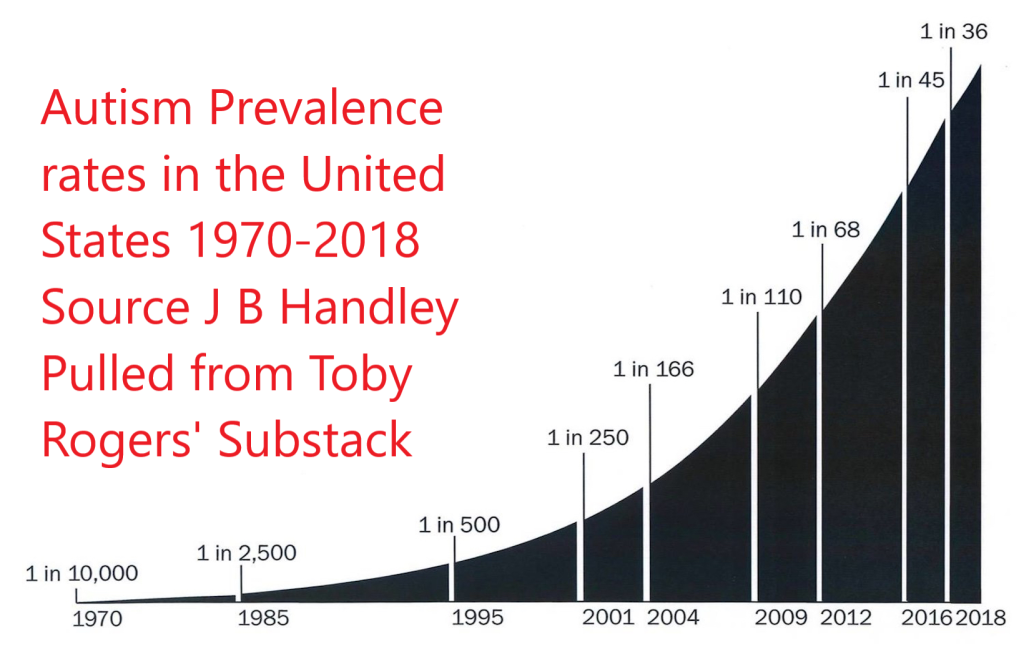



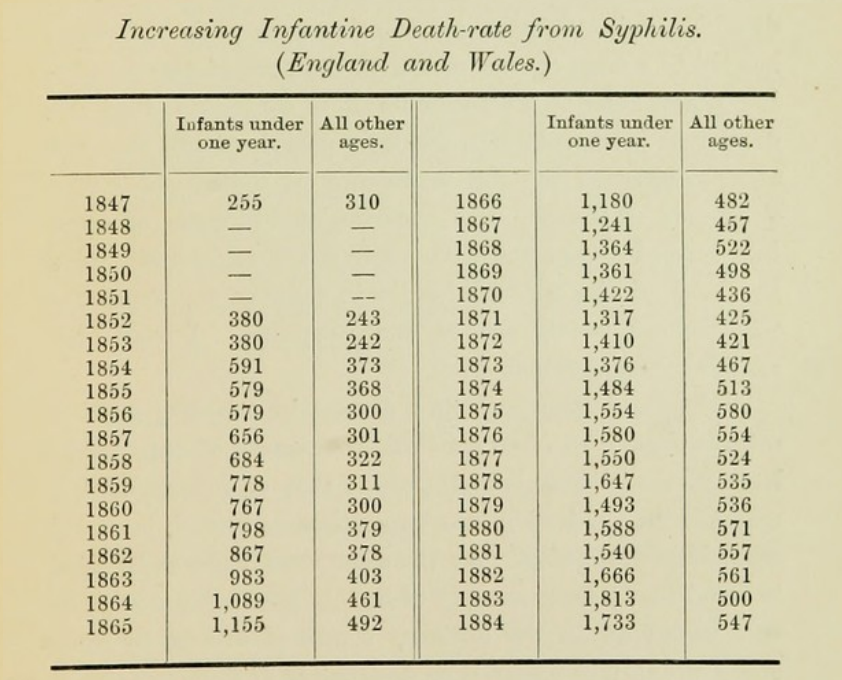

{kind=link}