The ‘Neurodiversity’ Industry Is A Cover for Vaccine Injury – Part II, Two Narratives
Introduction
Since the 1990s, the idea of ‘neurodiversity’ has become a cottage industry. The basic tenet of neurodiversity is that autism is a perfectly normal variation of human development that should not be seen as a negative trait. It seeks to highlight the alleged ‘positive’ traits of autism and believes that the struggles of people with autism are largely caused by society not being accepting rather than the inherent downsides of the condition. This article will seek to discuss three parts of this phenomenon by comparing two theories of autism: the neurodiversity theory of autism and the iatrogenic theory of autism i.e. vaccine injury. The first part will discuss the evidence for each theory, concluding that vaccine injury has a large amount of evidence to support it. The second part of this article will look at the individuals and institutions that promote each theory and how the media portrays each group. The third part will draw it together by explaining how the neurodiversity theory is constructed as an alternative to deflect from the vaccine injury theory and to gaslight people suffering with autistic vaccine-injury and their parents about their experiences.
This is part II of the three part series.
Part II: Two Narratives
Having made the case that vaccine-injury is an extremely plausible theory of autism, I will now examine the contrast between how advocates of the neurodiversity narrative and advocates of the vaccine-injury narrative have been treated by the establishment. Although the neurodiversity narrative claims to be countercultural and in opposition to the ordinary view of autism, in reality it is promoted by mainstream sources. On the other hand, vaccine-injury theorists – including those who have backed their theories up by significant evidence – have faced consequences from being smeared to the loss of their career.
Is Neurodiversity Countercultural?
The neurodiversity narrative claims to be countercultural. As it is a fairly recent narrative, it portrays itself as the up and coming new narrative to ‘reframe’ autism in a positive light. In fact, the article I quoted from in Part I makes this argument, comparing it to different theories of autism:
The mainstream perspective – the perspective that autism is caused by a genetic defect and should be cured by targeting the autism gene(s).
The fringe theory – the theory that autism is caused by environmental factors like vaccines and pollution and should be cured through addressing these factors.
This narrative takes aspects of the ‘social justice’ style narrative, where those that are marginalised by society are reframing themselves as positive actors, reframing what is considered as ‘negative’ by society as a positive.
Of course, there is a long history of narratives claiming to be counterculture, when in fact, they are nothing of the sort. A good example, that has some similarities with the neurodiversity ideology, is transgenderism. Transgender ideology claims that opposite sex impersonators are a marginalized group, whereas in reality those who oppose them are censored, sacked, and smeared. Men playacting as women are promoted, celebrated and glorified in the media, with any criticism deemed as bigotry. Pharmaceutical companies support this narrative for profit, and many sinister actors use it is as a means of promoting transhumanism.
So is the neurodiversity narrative really countercultural?
In general, the best way to check if a narrative is against the establishment is to look at what the establishment actually says about it. If the establishment contains a large amount of institutions promoting a particular narrative, and is spending a lot of money on promoting a particular narrative, then there is a reason for that. So let us examine what the interconnected establishment/media/NGO complex actually states about autism and neurodiversity. This will look at several different groups: autism charities, the media, the fiction industry and other significant actors.
Autism Charities and Consultancy
Although some people would like to consider charities to be not ‘establishment’ institutions, in reality large charities are part of the establishment. Their role in society is to advance narratives that benefit establishment interests, but while seeming as if they are independent advocacy groups.
To give an example already alluded to in Part I, the Alzheimer’s Society expresses some scepticism that aluminium accumulation in the brain is the cause of Alzheimer’s disease. To acknowledge this would be bad for the establishment, since it is (elite) human action that unleashed aluminium on the environment and caused high levels of exposure. Questioning aluminium exposure in this case might lead one to come to the conclusion that the establishment does not have a concern for human health. Furthermore, obscuring the reality in this case allows Big Pharma to sell expensive patented drugs for Alzheimer’s disease, rather than reducing exposure or reducing aluminium in the human body. Foreign policy is another area where charities can be demonstrated to serve elite agendas. For example, human rights organisations will focus on violations of, say, freedom of speech by ‘enemy countries’ such as Russia, while ignoring the same or worse by Western countries or allies such as Saudi Arabia.
Of course, the issue is even more explosive when it comes to questioning vaccines, since vaccination is essentially the cult of the modern age:
Vaccinating everyone on earth (the goal of the Gates Foundation, W.H.O., Pharma, and presidents of both political parties) has nothing to do with health; its sole function is to give atheists in the developed world a feeling of heroism that supplies them with a sense of symbolic immortality.
TOBY ROGERS
So what do autism charities – allegedly set up to help people with autism – have to say about autism and neurodiversity?
The National Autistic Society is the main autism charity in the United Kingdom.
On its ’causes of autism’ page, the National Autistic Society says this:
There is no known ‘cure’ for autism. We also believe that autism does not need a ‘cure’ and should be seen as a difference, not a disadvantage. We also warn people about fake cures and potentially harmful interventions here.
This does not mean that autistic people do not face challenges, but with the right support in place, they are more than capable of living fulfilling and happy lives.
This is, of course, the neurodiversity narrative. On the other hand they say that vaccines don’t cause autism, because that idea must be opposed at all costs.
If we look at the National Autistic Society’s funding, they have a turnover of large amounts of money. If we look at their funding for 2023 in their annual accounts, they have a list of companies who they give special thanks. They have funding from some large companies such as Coca Cola and JP Morgan Chase.
It is also worth noting that there is an entire industry of autism ‘consultancy’, which is designed to promote neurodiversity, particularly relating to employment. There are a whole bunch of services available, for example, Aspire Autism Consultancy provides “bespoke neurodiversity training for therapists and healthcare practitioners.”
It is also worth noting that if you do want accommodations at work related to autism as a disability, you are basically obliged to put up with the neurodiversity framing.
The Media
The mainstream media is another crucial plank of the establishment, that serves their interests. The purpose of the media is not to present the news in an objective way, but to be propaganda for the powers that be. The structure of the mainstream media goes through multiple filters and each one excludes any opposition voices to ensure a conformity of thought.
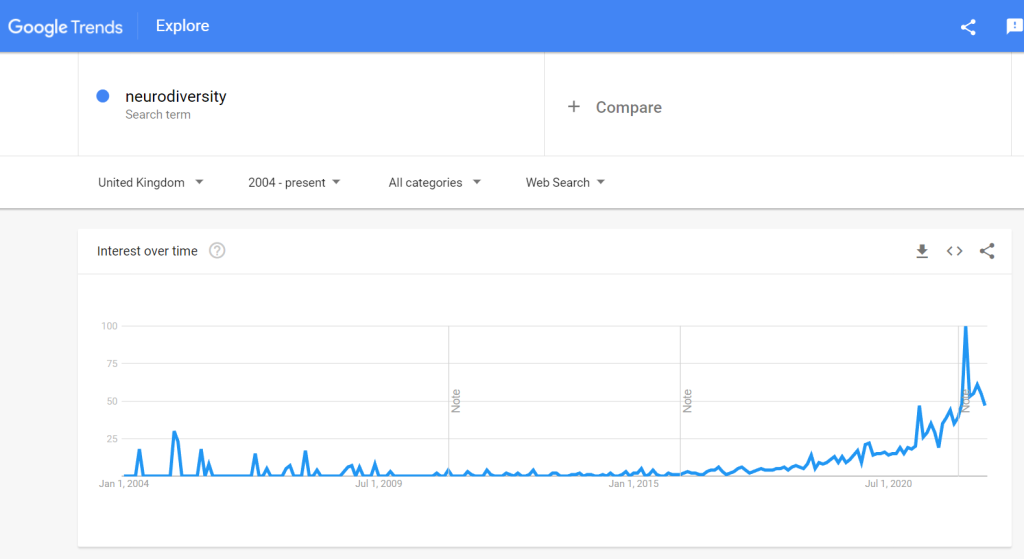
There are plenty of articles in the media promoting the neurodiversity agenda. A survey of the media carried out by pro neurodiversity activists found the following result (abstract only available):
Results showed increased coverage of neurodiversity and neurodivergent individuals from 2016 to 2022. Key findings include an increase in calls for representation, advocacy, and the recognition of neurodiversity as a different neurotype rather than a condition to be cured.
Recently in the UK, there has been a programme hosted by Chris Packham, and autistic man and advocate for neurodiversity about autism and ADHD (ADHD is also considered to be an example of neurodiversity by advocates, and is also possibly vaccination injury although, unlike autism there is not as much evidence to prove this). I haven’t watched the programme because I don’t want to waste the energy getting angry about the obvious misrepresentation of autism that will exist within the program. It is worth noting that the programme about autism was nominated for a television award, meaning that it must have been viewed as in line with what the media and establishment wish to promote. Articles in the media have also promoted this programme, and called it moving (even the more right leaning Telegraph, which is, say, more sceptical of similar ideologies like transgenderism).
The Fiction Industry
Fiction may seem as if it is separate from the establishment, but in reality the establishment has a significant influence here as well, particularly when it comes to television. For example, it is a well-known fact that a large number of American movies are produced with the help of the intelligence agencies.
If there are characters, action or dialogue that the DOD doesn’t approve of then the film-maker has to make changes to accommodate the military’s demands. If they refuse then the Pentagon packs up its toys and goes home. To obtain full cooperation the producers have to sign contracts, called Production Assistance Agreements, which lock them into using a military-approved version of the script. [emphasis in original text]
MINT PRESS NEWS
So how are autistic people portrayed in the media? There is but one model of the autistic film or TV character and that is the ‘autistic savant’. That is, someone who is socially inept but a genius at doing some weird obscure thing which wins the character the things that they want in life. In some portrayals a biting satirical wit might be added, particularly in comedy programs, with an edge of intellectual superiority played for laughs. Sheldon Cooper of The Big Bang Theory is the best example of this.
This is basically the neurodiversity model in action. Look at those special characters that think differently that have all these wonderful things like a PhD and an amazing job! No-one puts low functioning children who have to use a diaper and are non-verbal on the TV. No-one puts the 6′ 2″ 30-year-old man with a mental age of 5 who flies into incandescent, violent rages over sensory triggers on the TV. Why would they? So fiction gives an extremely misleading picture of autism to the public that bolsters the neurodiversity model.
Although neurodiversity advocates might also complain about the portrayal of autism in the media, the reality is that it is only their own ideology being reflected back at them. The special, unique one who ‘thinks differently’: that is their argument of what autism is, not mine, and that is their portrayal of what autism is, not mine.
Conclusion
As we can see from the above collection of evidence, the establishment has expressed a significant amount of support for neurodiversity.
The Vaccine Injury Approach to Autism and Its Critics
Vaccine-injury advocates have been treated rather differently by the establishment. This section will discuss a few different advocates of the autism-vaccination link: Dr. Andrew Wakefield, Dr. Christopher Exley, and Jenny McCarthy.
Dr. Wakefield Redux
The most obvious place to start on this topic is the demonisation of the British gastroenterologist, Dr. Andrew Wakefield. Dr. Wakefield is infamous among the vaccine pushers, and his name is invoked like that of the devil himself. Dr. Wakefield has been the subject of a thousand lies by the mainstream media and medical establishment. Eventually, he was struck off the medical register in 2010. His career was destroyed. So what was his ‘crime’? Simply to take parents seriously when they observed their children regressing into autistic behavior after the MMR vaccination.
So let’s look at how Dr. Wakefield got interested in the issue of the MMR vaccine and autism. After Dr. Wakefield performed studies on measles and gut issues, specifically Crohn’s disease, he was contacted by parents who saw their child regress into autistic vaccine-injury after their MMR vaccination. Dr. Wakefield and his colleagues at the Royal Free Hospital in the UK produced a case series of 12 of these children called, “Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children” published in the Lancet in 1998. Contra claims made by the mainstream media, which is to this day constitutionally incapable of representing this paper accurately, it was not designed to ‘prove’ that the MMR vaccine causes autism. The people who made the initial link between the MMR and autism were the parents of those children, not Dr. Wakefield.
Onset of behavioural symptoms was associated, by the parents, with measles, mumps, and rubella vaccination in eight of the 12 children, with measles infection in one child, and otitis media [ear infection] in another.
This eventually led to him being relentlessly attacked by Brian Deer, a Telegraph ‘journalist’ who was obsessed with destroying his career. Deer made multiple false claims about Dr. Wakefield and his study. These false claims included the claim that Wakefield and his colleagues did not have ethical approval for the medical testing that they ran on the ‘Lancet 12’ children and that Dr. Wakefield misrepresented the case histories of those children to push a narrative blaming the MMR vaccine. Deer also claimed that Wakefield had unethical conflicts of interest. As a result of these claims, Dr. Wakefield was eventually struck off the medical register in 2010. There is much more detail to this story not able to be discussed here for space considerations, so I suggest reading this article by Iain Davis if you would like a refresher on the full picture.
The mainstream media continues to promote false narratives about Dr. Wakefield to this day. Wikipedia, a so called ‘neutral’ encyclopedia, but that actually serves to promote establishment narratives, refers to him as being ‘discredited’ and ‘disgraced’ which means that you know the target is somewhere in the vicinity.
I will conclude by quoting Davis:
[Wakefield] is the sacrificial lamb and a stark warning to any scientist, medical practitioner or researcher who dares to challenge the corporate dictatorship. The MSM’s annihilation of Dr. Wakefield served two purposes. Firstly to convince a misinformed public that any who suggest vaccines may not all be wonder drugs are ‘evil’ and also to put the fear of God into the scientific community.
IAIN DAVIS – ‘THE EVISCERATION OF DR. ANDREW WAKEFIELD’
Dr. Christopher Exley
Dr. Christopher Exley is former Professor of Bioinorganic Chemistry at Keele University in the UK. He did his Ph.D. on aluminium exposure among fish and the harm that this can cause and is an extremely credible expert on the interaction of the neurotoxin aluminium with human and animal life. As shown above, he has studied the link between aluminium and autism (and other diseases such as Alzheimer’s disease and Multiple Sclerosis). He led the Aluminium Research Group and published around 200 papers on aluminium.
So what happened to Dr. Exley after he published his group’s paper on ‘Aluminium in Brain Tissue in Autism’?
The first thing to note is that the media has attacked Dr. Exley. The Guardian accused him of pushing ‘anti-vaccine misinformation’:
A British academic who has promoted anti-vaccine misinformation has raised more than £150,000 through a university donations portal to support his research during the coronavirus crisis, the Guardian can reveal.
They quote a vaccine promoter stating that Dr. Exley’s paper is ‘bad science’ but of course do not elucidate the audience about why it is bad science (the reader doesn’t need to know that, they just need to know which hate figure ‘anti-vaxxer’ of the week they need to condemn).
An even earlier hit piece from 2019 states:
Prof Chris Exley angered health experts for claiming that tiny amounts of aluminium in inactivated vaccines, such as the HPV and whooping cough inoculations, may cause “the more severe and disabling form of autism”.
They, of course, did this in order to try to make sure that the funding portals were shut down so the research could not continue (not that Keele needed any encouragement on this front – see below).
The case of Dr. Exley also reveals something else important about our media – the principle that experts are only experts until they question vaccination, then they become ‘misinformation’. Dr. Exley was an acceptable expert for the Guardian to cite when it came to the Camelford poisoning. This case involved aluminium was accidentally dunked into residents’ drinking water in Camelford in Cornwall. One woman, Carole Cross, died from a rare form of Alzheimer’s after this poisoning, with extremely high levels of aluminium in her brain. Dr. Exley is acting within his expertise by commenting on both cases, but only one is considered to be acceptable.
Keele University basically made Dr. Exley’s position at the university untenable for questioning the safety of aluminium adjuvants in vaccination.
Since that time [about 2015], the university has progressed from spiking Exley’s press releases and downplaying or ignoring major scientific contributions by Exley’s research group to — perhaps most concerningly — sabotaging the research donations that are the “lifeblood” of independent-minded scientists.
The University messed with his donations portal which he was using to crowdfund his research.
On the 11th of April 2019, following receipt of a number of emails from potential donors unable to make a donation using the online link, I was told by someone called Lee Bestwick in Finance that he had been instructed to disable the donations portal set up by Finance on my behalf. He was not aware that there had been no prior discussion with me about this.
We appreciate your interest in the University and in our research staff who are undertaking such a wide range of interesting and pioneering work, but hope you understand the delicate balance we must maintain to ensure our public and private reputation.
Kennedy wrote in response:
I must consider that your decision to return my personal check is likely the product of the pharmaceutical industry’s open, aggressive, and rather sinister campaign to defund Professor Exley. Vaccine makers view Dr. Exley’s efforts to accurately characterize, for the first time, the health impacts of aluminum adjuvants in vaccines, as a threat to their profit-taking. Terminating Professor Exley’s research has been a central objective of the $50 billion vaccine industry. This cartel wants the world to believe that aluminum in vaccines is safe despite the lack of any safety studies to indicate that is possible, and plenty of peer-reviewed literature that suggests that it is not.
Another Children’s Health Defense article states:
[A] recent letter to Exley from Keele University’s dean of natural sciences explained that “the university will no longer provide facilities to solicit or enable restricted charitable donations” to support the Exley group’s research on “the bioinorganic chemistry of aluminium and its links to neurodegenerative disease.”The dean clarified that this would include “donations from individuals, groups, charities and foundations” — amounting to the entirety of the group’s research income.
Eventually due to this disruption of funding the research group was shut down despite having around 200 peer reviewed publications.
Furthermore, Dr. Exley was suggesting methods by which to detox from aluminium and remove it from the body in order to reduce autistic symptoms. The method Dr. Exley suggested was drinking mineral waters with a high silicic acid content, as silicic acid binds to aluminium and then it is expelled from the body via urine. Again Dr. Exley demonstrated this through science, showing increased excretion of aluminium after consuming a litre of silica water. When done on a consistent basis (daily) this reduces the body burden of aluminium including in the brain and improvements in symptoms are observed (Dr. Exley witnessed this in Alzheimer’s disease). Not only was he showing what had harmed us, he was helping us with his protocol, and I can vouch that it works personally because I have tried it.
So now we can see that Dr. Wakefield is not the only person to lose his career for questioning the links between vaccines and autism.
Jenny McCarthy: Demonised Mothers
Jenny McCarthy is a media figure who spoke out about the safety of vaccination after her son, Evan, regressed into autism after receiving the MMR vaccine. McCarthy is different from the cases I have highlighted above in that she is the mother of a vaccine injured child. Her role as a mother affects her portrayal by the vaccine industry.
Generally speaking, mothers are considered less competent observers of their children than doctors, despite the fact that the doctor only sees the child for brief appointments and the mother is around the child 24/7. This is justified by the medical establishment, because they consider themselves to be the ‘experts’.
There is a significant amount of misogyny in the portrayal of McCarthy in the media. For example, news articles often introduce her as ‘former Playboy model Jenny McCarthy’ or other similar framing when talking about her scepticism of vaccination. The fact that McCarthy was involved in the pornography industry has no obvious relevant connection to her scepticism of vaccines. Except, in the mind of the vaccinationist, it is clearly related, since they always mention it.
The purpose of this framing is to invoke the Madonna-Whore complex, a misogynistic trope in which women are always the idealised, perfect mother, or the debased whore. Because McCarthy posed for Playboy, the implication is that she is inherently an unfit mother, unqualified to observe her son’s regression into autism. The other implication is that she is inherently stupid (women who have worked in pornography are perceived in society as ‘dumb bimbos’). Thus she is unable to correctly observe the behaviours of her own child in the mind of the vaccinationist.
Conclusion
Neurodiversity cannot be seen as an anti-establishment narrative. Like transgenderism, it is an ideology promoted by the establishment that pretends not to be promoted as such. In part III, we will discuss the target of the neurodiversity narrative – high functioning autistic people and parents of autistic children – and how this precludes vaccination criticism.



{kind=link}