Measles Pandemic!: The Latest Big Pharma Advertising Campaign

Introduction
The idea of ‘pandemics’ and ‘outbreaks’ is one of the most convenient and effective ways for a government to sell fear and make money for their corporate backers (via vaccination drives). Although this did happen before Covid-19, such with the 2009 H1N1 ‘pandemic’, after Covid-19 the media has focused more on viruses and ‘pandemics’ in general, with random scare stories about viruses being grist to the MSM mill. Over the past few weeks, the idea of a ‘measles pandemic’ has been heavily pushed in the UK media. This article will discuss three aspects of this phenomena: the narrative, the purpose and the reality.
Part 1: The Narrative
Back in around September/October 2022, I noticed there seemed to be several random articles in the mainstream media about the ‘low uptake’ on the MMR (measles, mumps, rubella) vaccine.
For example, this article in the Daily Mail:
More than a third of children have not had their life-saving MMR vaccine in parts of England, according to official stats which illustrate why health chiefs fear a measles resurgence.
Revealed: More than a THIRD of children have NOT had both MMR jabs in parts of England as uptake rates plunge to lowest level in a DECADE amid rise of anti-vaxx myths
Another article scaremongers about the risk of ‘outbreaks’:
Outbreaks of measles and polio are now ‘likely’, top experts warned today as official statistics revealed childhood vaccination rates have plunged.
Fears measles, polio and other ‘diseases of the past’ could return as child vaccination rates drop for ALL 14 inoculations – with MMR jab uptake at a DECADE low, ‘extremely worrying’ NHS statistics reveal
This immediately raised a red flag in my mind and got me thinking they might attempt to create a ‘measles pandemic’ and that this was the first signs of a new campaign.
Now, this narrative is back.
How are they building up the notion of fear?
The media has been recently filled with stories like this:
[T]he capital could experience an outbreak of between 40,000 and 160,0000 [yes, that typo is in the article] cases, fresh analysis by the UKHSA suggests.
London at risk of major measles outbreak, UK Health Security Agency warns
Let’s go a little bit deeper into the basis of this alleged measles outbreak:
UKHSA modelling suggests that, unless MMR vaccination rates improve, London could see a measles outbreak with tens of thousands of cases.
London at risk of measles outbreaks with modelling estimating tens of thousands of cases
Wait…modelling?
We all know how successful modelling was with Covid. That is, successful at selling fear, because it certainly wasn’t successful at predicting ‘Covid cases and deaths’ since all the data it came out with were massive overestimates.
The model pdf report says:
[T]he risk of widespread transmission of measles, leading to a measles epidemic across the UK is considered low.
Risk assessment for measles resurgence in the UK
After that caveat (not mentioned in the media) we get into some nice fear porn like this:
Hospitalisation rates vary by age but range from 20 to 40%.
20% of even the fittest and healthiest age groups would be hospitalised for measles? Who believes this nonsense?
There doesn’t seem to be much of a ‘model’ in the report, their argument seems to be the lower vaccination rate in London means that the R (remember R from Covid fear porn?) is approaching 1 and this means there could be an outbreak:
[U]sing the UKHSA model, the reproduction number in London is now close to or above 1 (R=1.6, R=1.4, R=0.91) and could therefore result in an outbreak of between 40,000 and 160,000 cases.
The R rate (that is, the rate at which a virus spreads in the community, if you don’t remember it from Covid, so 1 means every infected person infects 1 other person) is calculated purely from vaccination rates among 25 and under. So far yet, this is purely hypothetical as there is no mass measles outbreak.
As to why measles has been selected for the fear campaign?
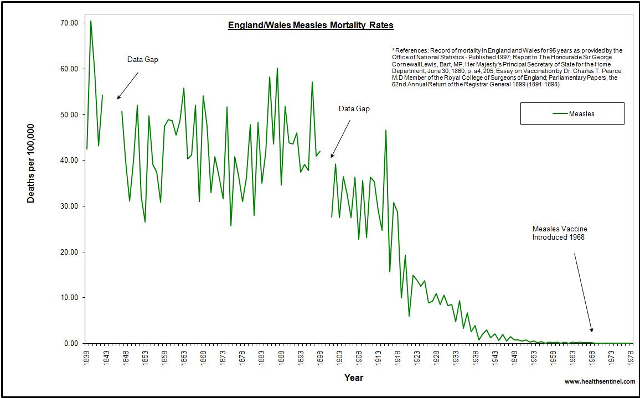
A measles outbreak seems a nice, likely candidate for a new fear campaign for a number of reasons. There is a large amount of (untrue) propaganda that a high mortality rate from measles was only stopped with the introduction of a measles vaccine.
Because measles is also a childhood disease, this evokes fear in parents that their child will die of measles. This contrasts with previous fear campaigns Covid-19, which clearly was not dangerous to children, and monkeypox/mpox/whatever-it-is-now, which largely affected gay men who had promiscuous sex.
Part 2: The Purpose

What’s the purpose of all this?
One of the main purposes is to sell MMR vaccination. Many of these articles fearmongering about measles (such as this one) have a picture of MMR vaccine vials – essentially product placement. You might not think the market would be that big – after all only young children get measles vaccines, right? But there’s actually potentially a bigger market than just young children available.
In fact, as per the UK Government, a large proportion of the population is not ‘fully vaccinated’ against measles, mumps and rubella. Why is this? Because the UK government deems that you need two doses to be ‘fully vaccinated’. The MMR vaccine (at 1 year) was introduced in 1988, but a second dose of the MMR vaccine (between 3-4) was not introduced until 1996, meaning 8 years of people not considered ‘fully protected’ who second doses can be sold to. Then there’s the people whose parents refused to let them have the MMR vaccination due to Wakefield’s paper. This group is referred to in the government press release as possibly ‘not fully vaccinated‘.
And then there are adults who were children before MMR was introduced. Presumably, these adults received a 1 dose measles single vaccine. Perhaps they are hoping that the endless fear porn will cause more people to ask their GPs for MMR vaccines. Many of the media articles stress that you can ask your GP about MMR vaccines if you are unsure of your vaccination status, as does the government press release:
Parents should check their children are fully vaccinated with 2 MMR doses, which gives 99% life-long protection, by checking their red book or with their GP practice, which younger and older adults can also do. Anyone not up-to-date should make an appointment as soon as possible.
London at risk of measles outbreaks with modelling estimating tens of thousands of cases
Another purpose is to demonise antivaxxers, and also to set up the narrative of blaming antivaxxers for any cases that occur (real or fabricated). We can see this in a recent article from the Daily Mail. Dr. Ahmad Malik, a British surgeon sceptical of the Covid jabs, recently interviewed Dr. Andrew Wakefield for his podcast. The Daily Mail immediately put out an article on Wakefield’s ‘misinformation’:
The disgraced ex-doctor and godfather of the anti-vax movement sparked fresh outrage today by claiming kids shouldn’t be given any jabs. Andrew Wakefield made the hugely controversial comments in a new podcast.
Disgraced ex-doctor and anti-vaxxer Andrew Wakefield claims he wouldn’t recommend kids get ANY jabs in new podcast, sparking fury among medics
While you do get occasional hit pieces on Wakefield in the media, why this podcast was selected for instant hatred was most likely due to the timing of its release – late July 2023. Wakefield has done multiple interviews with different alt-media (e.g. Steve Kirsch, UI Network, CHD) over the past few years without that much comment. However the timing of the release of the Malik podcast allows the media to blend this into their ‘measles pandemic’ push:
Fellow orthopaedic surgeon Dr Roshana Mehdian noted that Dr Malik was registered with the General Medical Council, the body that regulates medics in the UK. She noted that it comes ‘amidst a measles outbreak in London’.
Wakefield is ‘irresponsibly spreading’ ‘anti-vax disinformation’ ‘in the middle of an outbreak’ – where have we heard this tune before? This is a ‘measles outbreak’ that according to the article itself, consists of…85 cases.
The final function I will discuss is fear. That is pretty simple, to keep people in a state of fear so that if the government wants to revive policies like lockdowns in the future they will have an easier time of it. It has been demonstrated that people are more primed to accept authoritarian governments if there is a pandemic or illusion of a pandemic.
Part 3: The Problem
What do I mean by the problem? Vaccine failure. If we do get a resurgence of measles (which of course, is possible, although there is no evidence that this has occurred so far) vaccine failure will be the prime culprit.
The reality is that Measles/MMR vaccination has been a failure. The problem with vaccination is simple: while it is true that vaccination ‘produces antibodies’ the problem is that the manipulated solution of vaccination does not produce antibodies comparable to natural infection. This means that real immunity is not created to measles.
This is a study that Andrew Wakefield has pointed to in his discussions on measles vaccine failure. The study is called Measles Virus Neutralizing Antibodies in Intravenous Immunoglobulins: Is an Increase by Revaccination of Plasma Donors Possible? and it discusses levels of antibodies in blood donated for purposes of IVIG.
In short, levels of antibodies to measles are much lower since vaccination than they were prior to vaccination:

The study also found that adding a booster dose of the MMR vaccine only raises antibody levels in the very short term.
It’s also important to point out that all vaccination can do is put antibodies in the blood (regardless of the actual clinical meaning of those antibodies – as antivaxxers correctly argue, generating a bunch of antibodies is not proof of correlate of protection). The complex nature of the immune system is something not considered in vaccination (as discussed previously in this article). The complex responses created by natural infection are not something crudely rigging the immune system with vaccination can achieve. So if vaccination is even a failure at generation of blood antibody titers it’s a total failure.
James Lyons-Weiler also provided a helpful list of studies relating to measles vaccine failure on his substack. These are studies completed by vaccine promoters that nevertheless show real issues with measles vaccination. I cannot discuss all 25 (and of course, some of them are paywalled) but a glance at a few is worth our time.
One article from 1987 highlights vaccination failure was known even at that time:
An outbreak of measles occurred in a high school with a documented vaccination level of 98 per cent. Nineteen (70 per cent) of the cases were students who had histories of measles vaccination at 12 months of age or older and are therefore considered vaccine failures.
Measles outbreak in a vaccinated school population: epidemiology, chains of transmission and the role of vaccine failures.
One of the articles highlighted by Lyons-Weiler is co-written by Greg Poland, one of the most fanatical vaccinators on the planet. This is the guy who got tinnitus from the Covid ‘vaccine’, acknowledges he got tinnitus from the Covid ‘vaccine’ and still took a booster. So if even this guy is acknowledging limitations of measles vaccination, we must be looking at some degree of failure.
Receiving less attention, however, is the issue of vaccine failure. […][W]e and others have demonstrated that the immune response to measles vaccine varies substantially in actual field use. Multiple studies demonstrate that 2–10% of those immunized with two doses of measles vaccine fail to develop protective antibody levels, and that immunity can wane over time and result in infection (so-called secondary vaccine failure) when the individual is exposed to measles. For example, during the 1989–1991 U.S. measles outbreaks 20–40% of the individuals affected had been previously immunized with one to two doses of vaccine.
The Re-Emergence of Measles in Developed Countries: Time to Develop the Next-Generation Measles Vaccines?
For clarity we are talking about pretty small outbreaks here, so this as of yet cannot be taken as proof of mass vaccine failure. Nevertheless it demonstrates significant problems with the vaccine:
However, even with two documented doses of measles vaccine, our laboratory demonstrated that 8.9% of 763 healthy children immunized a mean of 7.4 years earlier, lacked protective levels of circulating measles-specific neutralizing antibodies [11], suggesting that even two doses of the current vaccine may be insufficient at the population level.
Meanwhile, the idea of measles ‘elimination’ via vaccination is a nonsense that is impossible, even with a mostly effective vaccine:
…measles eradication is unlikely as population immunity of 96–98% is required to prevent persisting measles endemicity [7,8,27,201]. In a recent study of measles-vaccine efficacy from 1960 to 2010, median efficacy was only 94% [28].
From an article by Poland, et al Cited by James Lyons-Weiler.
There are significant other factors concerning vaccine failure that could be considered, such as whether vaccination will drive new strains of the virus to arise, or that it may make measles more dangerous, that are beyond the scope of this article.
Conclusion
The UK government, media and establishment in general are attempting to push a fear based narrative around measles in order to sell MMR vaccination to the public and blame antivaxxers for any outbreaks. In reality, vaccine failure has been a contributing factor to outbreaks, and will continue to be so into the future.
Photo 1: by Markus Spiske on Pexels.com
Photo 2: Swab used in measles frequency studies, London, England, 1996 (salivette) by Unknown maker is licensed under CC-BY-NC-SA 4.0 (via Openverse)

