Think about what the CDC’s grotesque vaccine schedule does to the relationship between parents and their children. The kid does not know what’s going on. Yet every few months the parents offer up the child to strangers who inflict pain with sharp metal objects while smiling, laughing, and saying “it’s okay,” “you’re a champ.” The shots can cause fever, digestive problems, seizures, and worse for days, months, or even years. The parents go through this Molochian ritual over fifty times. The child has no words to express what’s happening. The child cannot possibly give consent. The psychological scars from this betrayal are permanent and the child learns to never trust the parents again.
Parents teach the idea of not following herd mentality. How many times have parents said “If so and so jumped off a cliff, would you?” to their children? How about this – if the white-coat told you to push your own child off the cliff, would you do it? Of course the answer is no, it’s only yes if the cliff is disguised as a sterile lighthouse shining light across the sea of disease. But nevertheless – if the white-coat told you, would you do it? Everyone is aware of the Milgram experiment. Vaccination is society’s Milgram experiment writ large, so insidious the authority of the white-coat that parents will destroy their own children.
Let’s see how this goes. A parent takes their child to be vaccinated, seeks the white-coat for the ‘well baby check-up’. Or perhaps not, perhaps the parent has some doubts about the shots, but the authority of the white-coat’s fanaticism removes this well enough. The child – probably in discomfort, fear, receives the holy baptism of the injection. However when they get home they aren’t right. They are having seizures, or a fever (dosed with paracetamol/acetaminophen no doubt, which aggravates the injuries). Then everything gets worse. The child stops speaking, stops making eye contact, loses skills. The white-coat gaslights the parent and claims the child was always this way, always damaged. The parent knows this is a lie, as there is nothing wrong with their memory.
The parent seeks those in the same boat with them, and the few doctors who will not lie to them about their children’s injury. They speak out about the child being vaccine-injured. They unite with other parents to tell the truth about vaccines. They promote and amplify doctors and experts telling the truth about vaccines. So far there is no problem: the gaslighting establishment medics need to be exposed as liars and frauds. Parents can give powerful testimony to the way their children were destroyed by vaccines.
So where is the problem?
The reality of the vaccine-injury movement – with the exception of the Covid ‘vaccine’, and to a lesser extent the Gardasil vaccine – is that the vast majority of those speaking are parents. This certainly applies very strongly to specifically autistic vaccine-injury. In part this is out of necessity: some autistic people are simply too severely vaccine-damaged to communicate regarding their injuries. In part this is out of the success of the ‘neurodiversity’ movement that convinces those with ‘high functioning’ autism that autism makes them special and unique and that there is nothing wrong with it. Nevertheless this necessity creates a skew, that those with are personally autistic vaccine-injured don’t get a voice or a prominent role in the vaccine-injury movement.
You can try this for yourself: when you think of people speaking about autism and vaccine injury, who first comes to mind? When I test this on myself, I come up with Robert F Kennedy, Jr, Andy Wakefield, JB Handley, Jenny McCarthy, Christopher Exley, Del Bigtree, you get the idea. No autistic people whatsoever. This creates a problem. Parents can articulate what they observe their child do and the distress of their child from the outside. Any medical professionals can describe what they have seen in injured children. Journalists can accurately describe the corruption. Doctors and journalists and advocates but no-one of any profile is doing this from the inside.
But now we must trespass on even more controversial territory, that is the question of guilt.
Does anyone else know what a paradox it is? That I can appreciate parents who speak out about their child’s vaccine injuries while feeling such bitterness and anger? To know that your parents love you but that they also ruined you for life?
And then this brings us to the most fundamental question: who is ruined? We can do this in a very simple way. Let’s use an example. Andy Wakefield has talked in interviews about the children in his 1998 Lancet study and how the parents of the vaccine-injured children were told that they should stick their child in a home, because ‘that’s autism’ and nothing could be done to help them. What is unsaid that – well fundamentally, that’s true. Not in the sense that nothing could be done to ease the child’s suffering, necessarily – but in the sense that the parent has the full capability to abandon their vaccine-injured child and walk away, whereas the child has no such luxury to abandon their vaccine-injuries. Don’t misunderstand me: I am not saying that this would be easy to do or would cause no distress to the parent. Just that it is possible: and therein lies the problem. The parent is intact: distressed, angry, feeling guilt, but nevertheless intact.
Parents of vaccine-injured children need to unconditionally be defended from the gaslighting mainstream medical establishment. I am happy to put my bitterness and anger aside for The Cause. After all, nothing matters more than making sure that there are no more human beings like me. But I will never be silent, and if there is a certain amount of discomfort in that refusal, then that is how it will have to be.
Since the 1990s, the idea of ‘neurodiversity’ has become a cottage industry. The basic tenet of neurodiversity is that autism is a perfectly normal variation of human development that should not be seen as a negative trait. It seeks to highlight the alleged ‘positive’ traits of autism and believes that the struggles of people with autism are largely caused by society not being accepting rather than the inherent downsides of the condition. This article will seek to discuss three parts of this phenomenon by comparing two theories of autism: the neurodiversity theory of autism and the iatrogenic theory of autism i.e. vaccine injury. The first part will discuss the evidence for each theory, concluding that vaccine injury has a large amount of evidence to support it. The second part of this article will look at the individuals and institutions that promote each theory and how the media portrays each group. The third part will draw it together by explaining how the neurodiversity theory is constructed as an alternative to deflect from the vaccine injury theory and to gaslight people suffering with autistic vaccine-injury and their parents about their experiences.
This is part II of the three part series.
Part II: Two Narratives
Having made the case that vaccine-injury is an extremely plausible theory of autism, I will now examine the contrast between how advocates of the neurodiversity narrative and advocates of the vaccine-injury narrative have been treated by the establishment. Although the neurodiversity narrative claims to be countercultural and in opposition to the ordinary view of autism, in reality it is promoted by mainstream sources. On the other hand, vaccine-injury theorists – including those who have backed their theories up by significant evidence – have faced consequences from being smeared to the loss of their career.
Is Neurodiversity Countercultural?
The neurodiversity narrative claims to be countercultural. As it is a fairly recent narrative, it portrays itself as the up and coming new narrative to ‘reframe’ autism in a positive light. In fact, the article I quoted from in Part I makes this argument, comparing it to different theories of autism:
The mainstream perspective – the perspective that autism is caused by a genetic defect and should be cured by targeting the autism gene(s).
The fringe theory – the theory that autism is caused by environmental factors like vaccines and pollution and should be cured through addressing these factors.
This narrative takes aspects of the ‘social justice’ style narrative, where those that are marginalised by society are reframing themselves as positive actors, reframing what is considered as ‘negative’ by society as a positive.
Of course, there is a long history of narratives claiming to be counterculture, when in fact, they are nothing of the sort. A good example, that has some similarities with the neurodiversity ideology, is transgenderism. Transgender ideology claims that opposite sex impersonators are a marginalized group, whereas in reality those who oppose them are censored, sacked, and smeared. Men playacting as women are promoted, celebrated and glorified in the media, with any criticism deemed as bigotry. Pharmaceutical companies support this narrative for profit, and many sinister actors use it is as a means of promoting transhumanism.
So is the neurodiversity narrative really countercultural?
In general, the best way to check if a narrative is against the establishment is to look at what the establishment actually says about it. If the establishment contains a large amount of institutions promoting a particular narrative, and is spending a lot of money on promoting a particular narrative, then there is a reason for that. So let us examine what the interconnected establishment/media/NGO complex actually states about autism and neurodiversity. This will look at several different groups: autism charities, the media, the fiction industry and other significant actors.
Autism Charities and Consultancy
Although some people would like to consider charities to be not ‘establishment’ institutions, in reality large charities are part of the establishment. Their role in society is to advance narratives that benefit establishment interests, but while seeming as if they are independent advocacy groups.
To give an example already alluded to in Part I, the Alzheimer’s Society expresses some scepticism that aluminium accumulation in the brain is the cause of Alzheimer’s disease. To acknowledge this would be bad for the establishment, since it is (elite) human action that unleashed aluminium on the environment and caused high levels of exposure. Questioning aluminium exposure in this case might lead one to come to the conclusion that the establishment does not have a concern for human health. Furthermore, obscuring the reality in this case allows Big Pharma to sell expensive patented drugs for Alzheimer’s disease, rather than reducing exposure or reducing aluminium in the human body. Foreign policy is another area where charities can be demonstrated to serve elite agendas. For example, human rights organisations will focus on violations of, say, freedom of speech by ‘enemy countries’ such as Russia, while ignoring the same or worse by Western countries or allies such as Saudi Arabia.
Of course, the issue is even more explosive when it comes to questioning vaccines, since vaccination is essentially the cult of the modern age:
Vaccinating everyone on earth (the goal of the Gates Foundation, W.H.O., Pharma, and presidents of both political parties) has nothing to do with health; its sole function is to give atheists in the developed world a feeling of heroism that supplies them with a sense of symbolic immortality.
There is no known ‘cure’ for autism. We also believe that autism does not need a ‘cure’ and should be seen as a difference, not a disadvantage. We also warn people about fake cures and potentially harmful interventions here.
This does not mean that autistic people do not face challenges, but with the right support in place, they are more than capable of living fulfilling and happy lives.
This is, of course, the neurodiversity narrative. On the other hand they say that vaccines don’t cause autism, because that idea must be opposed at all costs.
It is also worth noting that there is an entire industry of autism ‘consultancy’, which is designed to promote neurodiversity, particularly relating to employment. There are a whole bunch of services available, for example, Aspire Autism Consultancy provides “bespoke neurodiversity training for therapists and healthcare practitioners.”
It is also worth noting that if you do want accommodations at work related to autism as a disability, you are basically obliged to put up with the neurodiversity framing.
The Media
The mainstream media is another crucial plank of the establishment, that serves their interests. The purpose of the media is not to present the news in an objective way, but to be propaganda for the powers that be. The structure of the mainstream media goes through multiple filters and each one excludes any opposition voices to ensure a conformity of thought.
There are plenty of articles in the media promoting the neurodiversity agenda. A survey of the media carried out by pro neurodiversity activists found the following result (abstract only available):
Results showed increased coverage of neurodiversity and neurodivergent individuals from 2016 to 2022. Key findings include an increase in calls for representation, advocacy, and the recognition of neurodiversity as a different neurotype rather than a condition to be cured.
Recently in the UK, there has been a programme hosted by Chris Packham, and autistic man and advocate for neurodiversity about autism and ADHD (ADHD is also considered to be an example of neurodiversity by advocates, and is also possibly vaccination injury although, unlike autism there is not as much evidence to prove this). I haven’t watched the programme because I don’t want to waste the energy getting angry about the obvious misrepresentation of autism that will exist within the program. It is worth noting that the programme about autism was nominated for a television award, meaning that it must have been viewed as in line with what the media and establishment wish to promote. Articles in the media have also promoted this programme, and called it moving (even the more right leaning Telegraph, which is, say, more sceptical of similar ideologies like transgenderism).
The Fiction Industry
Fiction may seem as if it is separate from the establishment, but in reality the establishment has a significant influence here as well, particularly when it comes to television. For example, it is a well-known fact that a large number of American movies are produced with the help of the intelligence agencies.
If there are characters, action or dialogue that the DOD doesn’t approve of then the film-maker has to make changes to accommodate the military’s demands. If they refuse then the Pentagon packs up its toys and goes home. To obtain full cooperation the producers have to sign contracts, called Production Assistance Agreements, which lock them into using a military-approved version of the script. [emphasis in original text]
So how are autistic people portrayed in the media? There is but one model of the autistic film or TV character and that is the ‘autistic savant’. That is, someone who is socially inept but a genius at doing some weird obscure thing which wins the character the things that they want in life. In some portrayals a biting satirical wit might be added, particularly in comedy programs, with an edge of intellectual superiority played for laughs. Sheldon Cooper of The Big Bang Theory is the best example of this.
This is basically the neurodiversity model in action. Look at those special characters that think differently that have all these wonderful things like a PhD and an amazing job! No-one puts low functioning children who have to use a diaper and are non-verbal on the TV. No-one puts the 6′ 2″ 30-year-old man with a mental age of 5 who flies into incandescent, violent rages over sensory triggers on the TV. Why would they? So fiction gives an extremely misleading picture of autism to the public that bolsters the neurodiversity model.
Although neurodiversity advocates might also complain about the portrayal of autism in the media, the reality is that it is only their own ideology being reflected back at them. The special, unique one who ‘thinks differently’: that is their argument of what autism is, not mine, and that is their portrayal of what autism is, not mine.
Conclusion
As we can see from the above collection of evidence, the establishment has expressed a significant amount of support for neurodiversity.
The Vaccine Injury Approach to Autism and Its Critics
Vaccine-injury advocates have been treated rather differently by the establishment. This section will discuss a few different advocates of the autism-vaccination link: Dr. Andrew Wakefield, Dr. Christopher Exley, and Jenny McCarthy.
Dr. Wakefield Redux
The most obvious place to start on this topic is the demonisation of the British gastroenterologist, Dr. Andrew Wakefield. Dr. Wakefield is infamous among the vaccine pushers, and his name is invoked like that of the devil himself. Dr. Wakefield has been the subject of a thousand lies by the mainstream media and medical establishment. Eventually, he was struck off the medical register in 2010. His career was destroyed. So what was his ‘crime’? Simply to take parents seriously when they observed their children regressing into autistic behavior after the MMR vaccination.
So let’s look at how Dr. Wakefield got interested in the issue of the MMR vaccine and autism. After Dr. Wakefield performed studies on measles and gut issues, specifically Crohn’s disease, he was contacted by parents who saw their child regress into autistic vaccine-injury after their MMR vaccination. Dr. Wakefield and his colleagues at the Royal Free Hospital in the UK produced a case series of 12 of these children called, “Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children” published in the Lancet in 1998. Contra claims made by the mainstream media, which is to this day constitutionally incapable of representing this paper accurately, it was not designed to ‘prove’ that the MMR vaccine causes autism. The people who made the initial link between the MMR and autism were the parents of those children, not Dr. Wakefield.
Onset of behavioural symptoms was associated, by the parents, with measles, mumps, and rubella vaccination in eight of the 12 children, with measles infection in one child, and otitis media [ear infection] in another.
This eventually led to him being relentlessly attacked by Brian Deer, a Telegraph ‘journalist’ who was obsessed with destroying his career. Deer made multiple false claims about Dr. Wakefield and his study. These false claims included the claim that Wakefield and his colleagues did not have ethical approval for the medical testing that they ran on the ‘Lancet 12’ children and that Dr. Wakefield misrepresented the case histories of those children to push a narrative blaming the MMR vaccine. Deer also claimed that Wakefield had unethical conflicts of interest. As a result of these claims, Dr. Wakefield was eventually struck off the medical register in 2010. There is much more detail to this story not able to be discussed here for space considerations, so I suggest reading this article by Iain Davis if you would like a refresher on the full picture.
[Wakefield] is the sacrificial lamb and a stark warning to any scientist, medical practitioner or researcher who dares to challenge the corporate dictatorship. The MSM’s annihilation of Dr. Wakefield served two purposes. Firstly to convince a misinformed public that any who suggest vaccines may not all be wonder drugs are ‘evil’ and also to put the fear of God into the scientific community.
IAIN DAVIS – ‘THE EVISCERATION OF DR. ANDREW WAKEFIELD’
Dr. Christopher Exley
Dr. Christopher Exley is former Professor of Bioinorganic Chemistry at Keele University in the UK. He did his Ph.D. on aluminium exposure among fish and the harm that this can cause and is an extremely credible expert on the interaction of the neurotoxin aluminium with human and animal life. As shown above, he has studied the link between aluminium and autism (and other diseases such as Alzheimer’s disease and Multiple Sclerosis). He led the Aluminium Research Group and published around 200 papers on aluminium.
So what happened to Dr. Exley after he published his group’s paper on ‘Aluminium in Brain Tissue in Autism’?
The first thing to note is that the media has attacked Dr. Exley. The Guardian accused him of pushing ‘anti-vaccine misinformation’:
A British academic who has promoted anti-vaccine misinformation has raised more than £150,000 through a university donations portal to support his research during the coronavirus crisis, the Guardian can reveal.
They quote a vaccine promoter stating that Dr. Exley’s paper is ‘bad science’ but of course do not elucidate the audience about why it is bad science (the reader doesn’t need to know that, they just need to know which hate figure ‘anti-vaxxer’ of the week they need to condemn).
Prof Chris Exley angered health experts for claiming that tiny amounts of aluminium in inactivated vaccines, such as the HPV and whooping cough inoculations, may cause “the more severe and disabling form of autism”.
They, of course, did this in order to try to make sure that the funding portals were shut down so the research could not continue (not that Keele needed any encouragement on this front – see below).
The case of Dr. Exley also reveals something else important about our media – the principle that experts are only experts until they question vaccination, then they become ‘misinformation’. Dr. Exley was an acceptable expert for the Guardian to cite when it came to the Camelford poisoning. This case involved aluminium was accidentally dunked into residents’ drinking water in Camelford in Cornwall. One woman, Carole Cross, died from a rare form of Alzheimer’s after this poisoning, with extremely high levels of aluminium in her brain. Dr. Exley is acting within his expertise by commenting on both cases, but only one is considered to be acceptable.
Keele University basically made Dr. Exley’s position at the university untenable for questioning the safety of aluminium adjuvants in vaccination.
Since that time [about 2015], the university has progressed from spiking Exley’s press releases and downplaying or ignoring major scientific contributions by Exley’s research group to — perhaps most concerningly — sabotaging the research donations that are the “lifeblood” of independent-minded scientists.
On the 11th of April 2019, following receipt of a number of emails from potential donors unable to make a donation using the online link, I was told by someone called Lee Bestwick in Finance that he had been instructed to disable the donations portal set up by Finance on my behalf. He was not aware that there had been no prior discussion with me about this.
We appreciate your interest in the University and in our research staff who are undertaking such a wide range of interesting and pioneering work, but hope you understand the delicate balance we must maintain to ensure our public and private reputation.
Kennedy wrote in response:
I must consider that your decision to return my personal check is likely the product of the pharmaceutical industry’s open, aggressive, and rather sinister campaign to defund Professor Exley. Vaccine makers view Dr. Exley’s efforts to accurately characterize, for the first time, the health impacts of aluminum adjuvants in vaccines, as a threat to their profit-taking. Terminating Professor Exley’s research has been a central objective of the $50 billion vaccine industry. This cartel wants the world to believe that aluminum in vaccines is safe despite the lack of any safety studies to indicate that is possible, and plenty of peer-reviewed literature that suggests that it is not.
[A] recent letter to Exley from Keele University’s dean of natural sciences explained that “the university will no longer provide facilities to solicit or enable restricted charitable donations” to support the Exley group’s research on “the bioinorganic chemistry of aluminium and its links to neurodegenerative disease.”
The dean clarified that this would include “donations from individuals, groups, charities and foundations” — amounting to the entirety of the group’s research income.
Eventually due to this disruption of funding the research group was shut down despite having around 200 peer reviewed publications.
Furthermore, Dr. Exley was suggesting methods by which to detox from aluminium and remove it from the body in order to reduce autistic symptoms. The method Dr. Exley suggested was drinking mineral waters with a high silicic acid content, as silicic acid binds to aluminium and then it is expelled from the body via urine. Again Dr. Exley demonstrated this through science, showing increased excretion of aluminium after consuming a litre of silica water. When done on a consistent basis (daily) this reduces the body burden of aluminium including in the brain and improvements in symptoms are observed (Dr. Exley witnessed this in Alzheimer’s disease). Not only was he showing what had harmed us, he was helping us with his protocol, and I can vouch that it works personally because I have tried it.
So now we can see that Dr. Wakefield is not the only person to lose his career for questioning the links between vaccines and autism.
Jenny McCarthy: Demonised Mothers
Jenny McCarthy is a media figure who spoke out about the safety of vaccination after her son, Evan, regressed into autism after receiving the MMR vaccine. McCarthy is different from the cases I have highlighted above in that she is the mother of a vaccine injured child. Her role as a mother affects her portrayal by the vaccine industry.
Generally speaking, mothers are considered less competent observers of their children than doctors, despite the fact that the doctor only sees the child for brief appointments and the mother is around the child 24/7. This is justified by the medical establishment, because they consider themselves to be the ‘experts’.
There is a significant amount of misogyny in the portrayal of McCarthy in the media. For example, news articles often introduce her as ‘former Playboy model Jenny McCarthy’ or other similar framing when talking about her scepticism of vaccination. The fact that McCarthy was involved in the pornography industry has no obvious relevant connection to her scepticism of vaccines. Except, in the mind of the vaccinationist, it is clearly related, since they always mention it.
The purpose of this framing is to invoke the Madonna-Whore complex, a misogynistic trope in which women are always the idealised, perfect mother, or the debased whore. Because McCarthy posed for Playboy, the implication is that she is inherently an unfit mother, unqualified to observe her son’s regression into autism. The other implication is that she is inherently stupid (women who have worked in pornography are perceived in society as ‘dumb bimbos’). Thus she is unable to correctly observe the behaviours of her own child in the mind of the vaccinationist.
Conclusion
Neurodiversity cannot be seen as an anti-establishment narrative. Like transgenderism, it is an ideology promoted by the establishment that pretends not to be promoted as such. In part III, we will discuss the target of the neurodiversity narrative – high functioning autistic people and parents of autistic children – and how this precludes vaccination criticism.
Since the 1990s, the idea of ‘neurodiversity’ has become a cottage industry. The basic tenet of neurodiversity is that autism is a perfectly normal variation of human development that should not be seen as a negative trait. It seeks to highlight the alleged ‘positive’ traits of autism and believes that the struggles of people with autism are largely caused by society not being accepting rather than the inherent downsides of the condition. This article will seek to discuss three parts of this phenomenon by comparing two theories of autism: the neurodiversity theory of autism and the iatrogenic theory of autism i.e. vaccine injury. The first part will discuss the evidence for each theory, concluding that vaccine injury has a large amount of evidence to support it. The second part of this article will look at the individuals and institutions that promote each theory and how the media portrays each group. The third part will draw it together by explaining how the neurodiversity theory is constructed as an alternative to deflect from the vaccine injury theory and to gaslight people suffering with autistic vaccine-injury and their parents about their experiences.
Part I: Two Theories
There are two main theories of autism. The first theory states that autism is genetic, and the second theory states that autism is iatrogenic. The first theory is advocated by both people who think that autism is a good thing, and by those who think it is a bad thing. The latter group of people, who believe that autism is a net negative but who also believe it is genetic, will not be discussed in this article. Instead we will be comparing the ‘autism is a positive, genetic gift’ group (the ‘neurodiversity’ group) to the ‘autism is iatrogenic, largely caused by vaccination’ group (the ‘vaccine-injury theory’ group). Part I will outline these two theories and look at the evidence.
The Neurodiversity Theory of Autism
What is the ‘neurodiversity’ theory of autism? It can be summed up by saying that autism is not a disability, it is a difference that should be celebrated. If you search for ‘neurodiversity’ you can find all sorts of articles advocating for this. Here’s one picked at random:
Neurodiversity is a movement that wants to change the way we think about autism. It rejects the idea that autism is a disorder and sees it instead as a neurological difference: one with a unique way of thinking and experiencing the world.
The movement focuses on celebrating neurological diversity and championing the different world-views and skills that autistic, dyslexic, bipolar, and other neurodiverse people have.
The idea of ‘neurodiversity’ has been increasing in popularity as a paradigm to ‘explain’ autism.
Of course, saying that autism is a positive trait does not explain it. So neurodiversity theorists use genetics to explain autism.
I will argue that both sides of the neurodiversity coin are false: having autism is always a negative thing, and that genetics does not explain autism.
Let’s start with the genetics aspect. One significant piece of evidence that the autism-is-genetic advocates use is twin studies:
Since the first autism twin study in 1977, several teams have compared autism rates in twins and shown that autism is highly heritable. When one identical twin has autism, there is about an 80 percent chance that the other twin has it too. The corresponding rate for fraternal twins is around 40 percent.
On the surface, twin studies look like exceedingly convincing evidence. They have been used to argue for a genetic link for a varying range of problems, including schizophrenia. In reality, though, twin studies are not good evidence that autism is genetic.
The problem that we run into is that twins are likely to have had the same environmental exposure, and this is doubly true when it comes to vaccination. No parent is going to vaccinate one of their twins and not vaccinate the other in some sort of science experiment. Thus both twins will be getting very similar exposure to aluminium, thimerosal, etc. via vaccinations. (Though see this caveat: aluminium levels in vaccination can vary significantly when vials are actually examined). The other major issue with twin studies is that they conclude that interaction between the body and these kinds of exposures is ‘genetic’. A genetic propensity to, say, accumulate certain toxins may well exist in autism cases. But in order for autism to develop, exposure to the toxin is required, and exposure to a toxin is not genetic. The same weakness applies when looking at alleged genes that have been associated with autism – it could be that those genes simply predispose a person to toxin accumulation.
The main weakness in the genetic case for autism is below:
It goes without saying that human genes have not radically changed since 1970. So how can the autism rates have changed so drastically? Autism-is-genetic advocates have tried their best to explain this graph, but they have done a bad job of it, because the whole graph screams ‘environmental causes’. But let’s have a look at their explanations for an increase in autism.
The main explanation offered is that the definition of autism has got wider and that is why these numbers have increased so much. Intuitively, this is a really poor explanation, for a number of reasons. For a start, we are looking a massive, massive increase. 1 in 10,000 to 1 in 30 is huge. To explain this simply by stating ‘it’s increased diagnosis’ is intuitively and logically implausible. People who argue this, I think, don’t understand how large a proportion of the population 3% is. That is a very significant chunk of the population. Older people here can employ their common sense. Were 3% or more of your childhood colleagues autistic? If you doubt that you could tell, I assure you that you can with just a little thought. Poor eye contact is a dead giveaway for autism, as is just an obvious awkwardness. The reality is, even ‘high functioning’ autistic people just seem odd, weird and off in particular ways so I would say you could almost always tell. Furthermore, the unemployment rate for people with autism, according to UK government data, is 78%. If we approximate the data, if 1 in 30 people are autistic and 2/3 (being generous) cannot work, this means around 2% of the population cannot work due to autism. The idea that government institutions never noticed 2% of the population being unemployable due to autism is laughably implausible.
This hypothesis also does not fit the shape of the graph very well. It keeps curving upwards, rather than seeing a bump for a change in diagnostic criteria and a levelling. The graph has still not levelled off. At some point, you have to start asking questions.
This issue also becomes more difficult to cover up when you consider severe autism. Autistic people who have a basic level of functioning in the ‘real world’ may just come across to normal people as a bit weird. In these people’s case, it’s more possible that they may not have a diagnosis. This would not be the case with those with severe autistic deficits. Again this is another argument that is just absurd on the face of it:
You can’t have missed 97 percent of the children in the ’80s who had autism. They’re trying to get the public to believe that kids who spin in circles, don’t speak, don’t socialize, can’t go to the bathroom by themselves all existed in our public high schools and elementary schools in the ’80s but only today have gotten a proper diagnosis. It’s incomprehensible.
Aside from being intuitively implausible, one study on this issue concluded:
In summary, the incidence of autism rose 7- to 8-fold in California from the early 1990s through the present. Quantitative analysis of the changes in diagnostic criteria, the inclusion of milder cases, and an earlier age at diagnosis during this period suggests that these factors probably contribute 2.2-, 1.56-, and 1.24-fold increases in autism, respectively, and hence cannot fully explain the magnitude of the rise in autism.
But what about the claim that autism is always a net negative? Surely that’s a little bit fundamentalist? After all, some of the advocates of the neurodiversity theory are autistic themselves, right, and surely they would know? So let’s tackle this thorny question.
The most obvious piece of evidence to start with is life expectancy. The evidence demonstrates that autism significantly decreases life expectancy. This is pretty mainstream evidence that can be found with a quick search.
One study, published in the American Journal of Public Health in April 2017, finds the life expectancy in the United States of those with ASD to be 36 years old as compared to 72 years old for the general population.
In other words, according to this study autism halves life expectancy.
The other study was published by the British Journal of Psychiatry in January 2018. This was a Swedish study showing similar results but elaborating on other causes of death as well. This study showed a life expectancy in those with ASD with a cognitive disability (or a learning disability) at 39.5 years versus 70 years for the general population studied. Those with ASD without a learning disability had an average age of death at about 58 years.
Furthermore, most of these causes of death are inherent to autism. For example, being much more likely to die in an accident. Autistic people have poor motor control and are much more likely to have these kinds of accidents such as drowning that lead to death. Horrific anxiety at normal experiences, such as sensory issues around normal noise/light/smell stimuli, also increases mortality as the body becomes overwhelmed with the constant anxiety triggers, meaning that the body’s ability to fight cancers is impaired, and heart attack and stroke risk is increased. People with autism are also unemployed/unemployable, with only about 20% of autistic people even being employed in the UK. This is linked to having awful social skills, having severe anxiety, and in some cases being completely non verbal and non functional. Being perennially unemployable is bad for your health; higher unemployment rates have been well established to be linked to mortality in sociology.
A study that followed autistic people for 20 years showed even more negative outcomes, although most of the participants also had other intellectual disabilities.
The outcome data was grim, showing pervasive inability to live independently, hold a job, or manage money. Few became independent, with 99% unable to live independently. Of those, 70% lived at home with relatives, 21% lived in disability homes in the community, and 8% in residential facilities. A mere 3.7% attained postsecondary education, about half of those representing certificates from college disability programs. While the majority were considered incapable of holding a job in the competitive workspace, some worked in disability workshops or other sheltered positions. Most participants were incapable of handling money, even with caretaker assistance, with only 9.5% considered capable.
The neurodiversity paradigm likes to attempt to escape from this reality by claiming that this is purely down to ‘society’ refusing to accept us. That argument is nonsense. The argument is most obviously flawed when it comes to those with severe autism, since any range of accommodations will not fix deficits such as being non verbal, not being able to go to the toilet by yourself, seizures (comorbid with autism), extremely poor motor control, severe gastroenterological issues (linked to autism), sensory issues and meltdowns, etc. If a neurodiversity advocate would like to explain how ‘acceptance’ will fix these problems, the comment section is all theirs. But it is even pretty much nonsense when it comes to ‘high functioning’ autism as well. The reality is ‘acceptance’ and accommodations only really make a difference in edge cases when it comes to solving the issues outlined above. Take for example ability to work. The severely impaired autistic person will never be able to work, you can throw all the accommodations in the world at the issue, it’s not going to happen. Whereas, a high functioning or borderline high functioning autistic person may be able to work if given a few accommodations. I’m not arguing against accommodations. What I am arguing against is the idea that accommodations, or society being more accepting of autism will fix our problems. It won’t.
As for the supposed ‘positive’ aspects of autism, what are they? Usually, it is claimed that many people with autism are more intelligent and analytical than normal people. However, this is likely to confuse correlation and causation. The most plausible explanation here is that brain development is more likely to be disrupted by toxins in the case of intelligent people due to more dense neuron growth in highly intelligent people. And again, severe cases of autism are erased by this view. It glorifies a very narrow spectrum of individuals with autistic injury – the ‘autistic savant’ – while writing off the harms done to the rest.
So what about the people with autism diagnoses who make the claim that autism is a positive thing and that neurodiversity is valid? Well, if someone with an autism diagnosis saying something settles the question, then autism is a devastating vaccine-injury that destroys and obscures the true personality of the individual, rather than reflecting it. Because of course this author has an autism diagnosis. So this kind of argument gets us nowhere.
The Vaccine-Injury Theory of Autism
There is an alternative, ‘underground’ theory of autism which advocates for the view that autism is (at least primarily) caused by vaccination. This article will discuss one cause of autism that the author believes has been comprehensively documented, that is aluminium adjuvants in vaccination entering the brain, disrupting the housekeeping cells of the brain (glia and microglia)and triggering inflammatory reactions such as the il-6 pathway. This is not to say that there are no other problems with vaccination as it relates to autism or no other possible causes (e.g. thimerosal). This article will stick to one cause for reasons of length and clarity.
I will go into a little bit more detail on the basic theory, before discussing the evidence. Aluminium is used in ~80% of vaccines as an adjuvant (substance used to promote an immune response). It is in the vast majority of childhood vaccines, excluding the MMR. However, aluminium is also a neurotoxin that the body cannot filter out effectively when injected, and because of this it can enter the brain. In short, the mechanism of how the injury occurs is like this. The aluminium in a vaccine is injected into the body. Immune cells are stimulated to respond to the site of injection. These immune cells (macrophages) respond and ‘swallow’ the aluminium. But when any inflammatory event in the brain occurs, these cells will be called upon to help, but instead will bring a massive payload of toxic aluminium with them into the brain.
A set of nine criteria used to determine the strength of an association between a disease and its supposed causative agent. They form the basis of modern medical and dental epidemiological research.
The more of the Bradford-Hill criteria you can demonstrate, the more likely it is that A causes B. Let’s look at these criteria with relevance to the fact that vaccines cause autism.
The first factor we can discuss is coherence. In other words, “does the association fit with other facts?” In the case of the above theory, it fits very well with facts about aluminium.
Aluminium is toxic to the human body. Aluminium has no biological function in human life and so its presence in the human body is always a net negative. The idea than aluminium, at least, can be toxic is widely accepted. Furthermore, it is accepted that aluminium can enter into brain tissue. Even more than this, it is accepted that it can cause harm once it gets into the brain tissue. One form of aluminium toxicity where this occurs has been observed in dialysis patients:
[A]luminium toxicity occurs due to contamination of dialysis solutions, and treatment of the patients with aluminium-containing phosphate binding gels. Aluminium has been shown to be the major contributor to the dialysis encephalopathy [“damage or disease that affects the brain”] syndrome and an osteomalacic component of dialysis osteodystrophy.
In stating this so far, I haven’t deviated from accepted science. Slightly more controversial than this is the idea that Alzheimer’s is caused by aluminium in the brain. This idea has been around since 1965 according to the Alzheimer’s Society. Although some people doubt the correlation-causation relationship (I would argue more for financial reasons than scientific), there is evidence from a wide range of sources.
The Scotsman reported on a study performed by researchers looking at aluminium levels in drinking water that found people in areas with higher levels of aluminium were more likely to die of dementia. The study’s author said:
We still see this well accepted finding that higher levels of aluminium in particular are associated with an increased risk of dementia. It’s confirmatory rather than anything else. [my emphasis]
Dr. Chris Exley has done multiple studies showing high levels of aluminium in the brains of those who died with a diagnosis of Alzheimer’s disease.
Animal studies also provide further evidence for the fact that aluminium in injurious to the brain. Dr. Christopher Exley observed, when he was studying fish, that when the fish were exposed to aluminium, they would start hanging out in the corner of the tank. Another study, performed by a sheep farmer (and shown in the Bert Ehgartner documentary, Under the Skin), showed that sheep injected with aluminium adjuvant (even without an antigen) showed much higher levels of aggressive behaviour and did things like grind their teeth on metal railings. Mice are also negatively affected by aluminium:
Male mice in the “high Al” group showed significant changes in light–dark box tests and in various measures of behaviour in an open field. Female mice showed significant changes in the light–dark box at both doses, but no significant changes in open field behaviours.
Thus, aluminium was clearly affecting the neurochemistry of the animals, and these behaviours are decent proxies for autistic symptoms in humans (aggression being analogous to autistic meltdowns and the fish acting strangely being analogous to social avoidance).
All of this evidence is a strong case that the aluminium factor in autism is coherent. We know aluminium is toxic and can harm the brain. Therefore that it can cause the kind of behavioural issues that we observe in autism cannot be prima facie ruled out. This is Criteria 1 on our Bradford Hill list solidly met.
The next criteria we can discuss is dose-response relationship. In short, if we give more aluminium adjuvants to children, do we see an increase in autism? Recall our graph from above – the 1-in-10000 to the 1-in-36 increase in autism prevalence. Now let’s compare this to the increase in aluminium adjuvants and thus exposure.
Shaw and Tomljenovic wrote a paper addressing this topic:
By applying Hill’s criteria for establishing causality between exposure and outcome we investigated whether exposure to Al from vaccines could be contributing to the rise in ASD prevalence in the Western world. Our results show that: (i) children from countries with the highest ASD prevalence appear to have the highest exposure to Al from vaccines; (ii) the increase in exposure to Al adjuvants significantly correlates with the increase in ASD prevalence in the United States observed over the last two decades (Pearson r=0.92, p<0.0001); and (iii) a significant correlation exists between the amounts of Al administered to preschool children and the current prevalence of ASD in seven Western countries, particularly at 3-4 months of age (Pearson r=0.89-0.94, p=0.0018-0.0248).
The correlation here is strong – more doses, more autism. The dose-response relationship is in this data. Point 2 on the Bradford Hill Criteria list is met.
The third factor that we can discuss is strength of association. Or in other words, how much is the difference in observed rates of autism between the vaccinated and the unvaccinated? This question is not all that easy to answer, mostly because information on this kind of question has been suppressed.
Dr. Paul Thomas has revealing evidence on this question.
Dr. Paul Thomas is the most successful doctor in the world at preventing autism. Data from his practice show:
If zero vaccines, autism rate = 1 in 715;
If alternative vaccine schedule, autism rate = 1 in 440;
If CDC vaccine schedule, autism rate = 1 in 36.
[…]His alternative vaccine schedule reduces autism risk by more than 1200%. However even an alternative vaccine schedule increases autism risk by 160% versus no vaccines at all.
The difference between 1 in 715 and 1 in 36 is huge. This is evidence of a significant strength of association between two factors. Of course the historical evidence showing fewer cases of autism among older people and more among the young with a strong correlation also matches up with this evidence, since older people are comparatively ‘unvaccinated’. So that’s our third criteria met.
The fourth factor we can discuss is temporal relationship. In other words, the effect must follow, not precede exposure. This factor is difficult to elucidate with vaccines, because exposure is so early on in life, including in the first day of life in the US. This is used by the vaccine cult to argue for the genetic position, but also ensures that it is more difficult to prove that exposure causes the symptoms because the exposure is so early and rampant. However, the simple observation of vaccines preceding autism is almost always true (unless the child is unvaccinated) because if you expose the child at day 1 (US) or 2 months (UK) that is before autistic behaviour is observed. So in a way, their rampant pushing of vaccinations has met this criteria all by itself.
We also haveanecdotal evidencefor this factor, that is, parents observing their child regressing into autism after vaccination. Of course, anecdotal evidence is automatically dismissed by any Pharma apologist. It is true that when using anecdotal evidence, there are significant pitfalls to consider. People can misremember things, or actively lie. These points are worthy of consideration.
However, both of these risks are minimised in the case of assessing autistic regression after vaccination. In terms of lying, there is simply no motive for a parent to lie about observation of regression into autism after a vaccine. Suggesting to a paediatrician, for example, that a child’s autism was caused by a vaccine will lead to being attacked and dismissed by the doctor. Parents are also attacked in the media if they suggest this idea, such as in the case of Jenny McCarthy, who has been subject to hit pieces because she stated that the MMR vaccine caused her son’s autism. Although vaccine advocates state that parents are likely to fall for the idea that someone is to blame for their child’s autism (such as doctors or Pharma) this is also unlikely. The parents had to consent for the vaccine to be given, and so you would expect to observe the opposite: parents denying that vaccines cause autism, since then they would have to blame themselves for consenting to the vaccine(s) and human beings do not like to acknowledge guilt.
Being mistaken about observation is also less likely in the case of autistic regression. This is because we are talking about parental observation of children and decent parents are highly alert to any signs of illness in a child, particularly a child of the age likely to receive vaccines. I will concede however that it is not impossible for someone to either be mistaken or lie. However it is quite implausible that given the factors weighing against these that all cases are examples of lying or misremembering given the multitude of testimonies that we have.
Thus there is at least some evidence for criteria four on the Bradford-Hill list.
The fifth factor that we can discuss is consistency. In other words, if we introduce aluminium adjuvants to all sorts of different groups, rich, poor, black, white, Asian, male, female, etc, do we see increased levels of autism?
There is a male-female disparity in autism diagnosis, with males being significantly more likely to be diagnosed than females. There is likely some biological reason why boys are more susceptible to this form of aluminium poisoning that is currently unknown (or at least, unknown to me). Nevertheless we see an increase in autism diagnosis in both groups.
The sixth factor we can discuss is experimental evidence. In other words, do we have any hard evidence for aluminium in the brain in autism? The answer to this is yes.
Dr. Exley and his research team examined this question directly. They obtained samples of brain tissue from individuals that had died with a diagnosis of autism. This was the first study of this kind. They examined this brain tissue and found very high levels of aluminium in all samples.
The aluminium content of brain tissue in autism was consistently high. The mean (standard deviation) aluminium content across all 5 individuals for each lobe were 3.82(5.42), 2.30(2.00), 2.79(4.05) and 3.82(5.17) μg/g dry wt. for the occipital, frontal, temporal and parietal lobes respectively. These are some of the highest values for aluminium in human brain tissue yet recorded and one has to question why, for example, the aluminium content of the occipital lobe of a 15 year old boy would be 8.74 (11.59) μg/g dry wt.?
We can add another one of Exley’s papers to make this evidence even better. This paper by Exley and Clarkson contains control samples who died with no signs of neurodegenerative disease:
The aluminium content of each lobe (mean and SD) were 1.03 (1.64), 1.02 (1.27), 0.95 (0.88), 0.77 (0.92) and 0.51 (0.51) μg/g dry wt.
These samples have much lower levels of aluminium in them than the autism samples, and this is despite the fact that the controls were mostly older than the autism samples – meaning lifelong exposure to aluminium through non-vaccine routes would have been higher and it would have had more time to accumulate in the control tissues.
The main limitation of this evidence as pointed out by its critics is that the study had a small sample size of N=5 when it came to measuring aluminium concentration in the autism samples (and for some aspects of the study N=10). This was for practical reasons (i.e. there isn’t a large amount of samples of autistic brain tissue available).
It is fair to acknowledge this, and obviously it would be better if the sample size was larger. However, it is completely dishonest to dismiss this study because of the small sample size. This study, for example, is completely different from a survey where 5 participants answering would be worthless. We are looking at pathological brains with clear evidence of a high level of a neurotoxin in them. The level of neurotoxin in these brains cannot be explained away by saying that there is only a few of them. To have that level of brain aluminium content and for it to not be pathological and negatively affecting the cells around it is absurd, unless you want to straight up deny that aluminium is neurotoxic.
Furthermore, no-one has tried to either confirm or reject the Aluminium Research Group’s findings (to this author’s knowledge at least). The establishment haven’t done a study where they demonstrate that the levels of aluminium found by the group are overly high. This is another case where the establishment claim the evidence isn’t good enough to support an anti-establishment view and then just ignore the question. So, despite establishment criticisms, this is criteria six on our Bradford-Hill list met.
We can use Exley’s evidence to discuss the seventh criteria, biological plausibility.
The 2018 paper shows that the high levels of aluminium were found associated with glia and microglia:
Discrete deposits of aluminium approximately 1 μm in diameter were clearly visible in both round and amoeboid glial cell bodies (e.g. Fig. 3b). Intracellular aluminium was identified in likely neurones and glia-like cells and often in the vicinity of or co-localised with lipofuscin (Fig. 5). Aluminium-selective fluorescence microscopy was successful in identifying aluminium in extracellular and intracellular locations in neurones and non-neuronal cells and across all brain tissues studied (Fig. 1, Fig. 2, Fig. 3, Fig. 4, Fig. 5).
This is important because those cells are disrupted in autism. For example, they are responsible for synaptic pruning, which does not occur correctly in autism.
Aluminium-loaded mononuclear white blood cells, probably lymphocytes, were identified in the meninges and possibly in the process of entering brain tissue from the lymphatic system (Fig. 1).
The eighth criteria we can discuss is specificity. The idea of specificity ideally means that one disease has one cause, but this is difficult to apply to reality as Bradford Hill acknowledged. Aluminium adjuvants, in reality, are highly likely to cause more than one disease. However, the argument is not just that aluminium adjuvants cause autism, but that a specific action of aluminium adjuvants causes autism. Our theory offers a specific toxicant (aluminium), a specific route of exposure (injection), a specific method by which that toxin gets into the brain (macrophages), specific cells that are disrupted (glia and microglia), and specific negative cascades that are triggered (excessive IL-6 production due to an inflammatory response). Our argument also does not claim that glial disruption by aluminium adjuvants causes a whole host of problems, but autism specifically (and nothing else). So the theory meets criteria eight on the list.
The last factor we can discuss is analogy. If we can observe similar things happening that makes our own theory more likely to be true. This is easy to demonstrate in the case of aluminium poisoning, as poisoning by different metals, such as mercury, can cause significant impairments in child functioning. One interesting case worthy of discussion here is that of acrodynia. Acrodynia, or ‘Pink disease’ was an early 20th century disease that symptomatically had some overlap with autism although with some differences. It was later proven that pink disease was a form of mercury poisoning caused by mercury teething powders. We know from this case that metal poisoning can cause symptoms with some similarities to autism. There are also examples of aluminium itself causing other forms of poisoning, which were discussed in point 1. So analogy also supports our case and gives us point 9.
Conclusion
As we can see from the above discussion, the idea that vaccines cause autism is strongly evidenced. However, the theory is also opposed by the entire establishment despite this evidence. It is to how these two differing theories of autism are treated that we now turn.
This article isn’t serious. It’s just taking the piss. We are going to break down a couple of articles from the MSM about one of their hate figures Dr. Andrew Wakefield. As we shall see, the media’s propaganda is pathetic, but you don’t need me to point that out. I’m just trying to be funny. (And I felt like some media arseholes deserved my undying scorn). I wrote this a while ago but because I am currently overwhelmed with crap I am struggling to finish research on more topics. So you all can have this instead.
Speaking in the measured, authoritative tones of an expert,
Yeah cos he is one.
Andrew Wakefield delivered his considered judgment on the coronavirus pandemic.
I have no doubt his judgement is more ‘considered’ than the people screeching about how we were all gonna die and posting feverish ‘case’ counts every day as if that shit was relevant to anything. (Remember when they did that in 2020? It seems surreal.)
For Wakefield, it’s not just an alarming time but also a heartening one. A poll found nearly a third of British people are either unsure or definitely wouldn’t take a vaccine for coronavirus.
You don’t need to support Andrew Wakefield to figure out that taking a product rushed to market based on a new technology never used on mass scale in humans before is kind of a bad fucking idea.
The survey was conducted for the Centre for Countering Digital Hate, which also found that almost 60 million people in the UK and U.S. subscribe to anti-vaxxer content on social media.
The Centre for Countering Digital Hate, you mean, the organisation who is less than transparent with who funds them, according to Dr Joseph Mercola? That one? Besides, what has ‘hate’ got to do with anything? If I state, “All vaccines are dangerous” what is ‘hateful’ about that? When I think of hate, I think of the Azov Battalion or something – oh no wait, sorry, they are now the Heroes Of Ukraine, I wasn’t up to date there with the latest Official Narrative, I apologise.
For the so-called anti-vaxxers
Funny you say ‘so-called’ because it’s generally you guys who call people that (even if they are not anti-vaxxers).
— for whom Wakefield remains a hero —
Yeah, so?
a world forced to communicate largely on the internet is a world particularly vulnerable to their scientific lies and twisted conspiracy theories.
Whose fault is that? Maybe you should have predicted that in Event 201. (They probably did predict that in Event 201).
During a ‘health freedom’ summit in May, Wakefield, the boyfriend of supermodel Elle ‘The Body’ Macpherson, looked cool and relaxed in a black yoga T-shirt as he chatted by video link to an adoring blonde interviewer.
Why is the interviewer’s hair colour relevant to this discussion? Outside of ‘haha look at the thick blonde bimbo’ garden variety misogyny?
‘One of the main tenets of mandatory vaccination has been fear, and never have we seen fear exploited in the way we do now with the coronavirus infection,’ he said.
Citing what he called ‘unambiguous’ evidence that the coronavirus is no more deadly than seasonal flu, and claiming that the pathogen’s death toll had been greatly exaggerated, Wakefield said the crisis had led to ‘a destruction of the economy, a destruction of people and families, and unprecedented violations of health freedom… and it’s all based upon a fallacy’.
Literally none of that is false.
I thought you were supposed to be making the case that Wakefield is a ‘conspiracy theorist’?
Describing vaccines as ‘intrinsically unsafe’,
True. Every single Big Pharma drug can cause significant harm to people who are susceptible to harm from that particular intervention. Vaccines aren’t exempt because magical fairy dust.
(I mean, I’d go a lot further than that, but you don’t need to for the statement to be true).
this valiant truth-teller called on free-thinking people to refuse to be vaccinated against Covid-19 if and when a jab becomes available.
If you are going to be as much of an idiot as you obviously are, don’t try the sarcasm game. Leave that to me.
‘If?’ lol as if they were ever going to let us off the hook by not introducing a vaccine.
Convincing his disciples that he was the victim of a conspiracy by the pharmaceutical industry, medical establishment and media, Wakefield now neatly argues that the same shadowy cabal are lying to the public about coronavirus.
“His disciples”? Seriously?
Having terrified one generation of parents — leading, some believe, to a spike in measles among children and a number of deaths in countries where a minority have promoted his claims — Wakefield is spreading fear and misinformation again.
Yeah guys Andy Wakefield is spreading fear. Not the guys who told you, ‘act like you’ve got it, don’t kill your grandma, cases are skyrocketing, hospitals are overwhelmed, we’re all gonna die’, they were just being rational and level headed and objective.
Critics also dismiss their hysteria about ‘compulsory’ vaccination as a red herring: this is illegal in Britain and has not been proposed in America.
Yeah this didn’t age well.
Interviewed for a TV series misleadingly called The Truth About Vaccines, Wakefield claimed that vaccines ‘are going to kill us’
This didn’t age well either. Yeah you might wanna google ‘died suddenly’.
Wakefield is handsome, charismatic and charming, and it’s no coincidence most of his supporters are women, often well-educated and well-heeled mothers.
Yeah, those women don’t support Andrew Wakefield because they saw their child regress after a vaccine and know what they saw, and he is one of the few people who will acknowledge that what they saw is real while the whole world tells them ‘it wasn’t the vaccine’. They just support him because they are sexually attracted to him. Amazing ‘logic’ on display from this writer.
While credulous celebrities are not exactly thin on the ground, anti-vaxxers have been delighted to welcome a more valuable ally in their efforts — an immunologist at University College Dublin named Prof Dolores Cahill. Dismissing the ‘hysteria’ over the pandemic, Cahill claimed that if people boosted their immune system with vitamins C and D and zinc supplements, 99 per cent could experience ‘just normal flu symptoms’ from Covid-19 and then be immune to the virus.
Cahill promoting the ‘conspiracy theory’ that Vit C, D, And Zinc improve the immune system. You can’t even take the piss out of this, it’s so ridiculous.
She further claimed that vaccines contain harmful ingredients such as aluminium or mercury
This quote doesn’t specify ‘vaccines’ for Covid – is the author of this article seriously trying to pretend vaccines don’t contain aluminium when it’s literally the adjuvant in most vaccines and that this fact is some sort of nutcase ‘claim’ by Cahill?
(and yes some of them still have mercury)
Wakefield lends arguments to people exasperated by the lockdown seeking to justify their rebellion against it, said Tara Smith, an infectious disease expert at Kent State University in Ohio, who has researched the anti-vaccine movement.
I have autism and I support Andrew Wakefield, research that. I’d like to see your theories on that one, go ahead.
Actually scratch that, I know what your theory would be. That I am just ‘self-hating’ and just need to see the magical land of neurodiversity and then I would live happily ever after. I’d still like to see you peddle it for a laugh though.
She wasn’t remotely surprised that Wakefield has latched on to coronavirus.
Wakefield didn’t have to ‘latch onto’ shit. You shoved Covid down our throats 24/7 for 2 years. Of course the whole world was bloody commenting on it at that point!
‘He has a huge following, it’s almost cult-like. Despite everything he’s done, they adore him.’
Yeah, it’s antivaxxers that are in a cult. Obviously.
The latest figures show only 89.2 per cent of one-year-old children received their first dose of the MMR jab in 2021-22, down from a peak of 92.7 per cent in 2013-14. It was the first time the figure had fallen below 90 per cent since 2010-11. Uptake of the second dose also fell to the lowest level in a decade at 85.7 per cent. Both doses are needed for full protection. [my emphasis]
When the MMR was first introduced [1988 in the United Kingdom] there was only one dose. Hence, I only had one dose of the MMR vaccine (that’s enough of that poison, thank you) – I guess I’m not ‘fully protected’ against measles, mumps and rubella. My life is still fucked though because of this poison (most likely the Pluserix vaccine they literally stopped using because it was too fucking dangerous as well, see image below and my post on Urabe vaccines) and I’m not even ‘fully protected’. Thanks for that, vaccine fanatics, go fuck yourselves.
Of course, no one else will bring up the fact that the only reason they had to introduce another dose is because the ‘protection’ from the MMR isn’t effective. Oh, don’t think it’s just the Covid jabs where they keep adding more doses! No!
The latest survey of 1,485 parents with children aged under four by the UK Health Security Agency found that 91 per cent think vaccines are safe. It also found 15 per cent of parents had seen on social media, or heard through friends, something that made them worried about their child being vaccinated.
Only 15%? Need to up our game, antivaxxers!
This suggested a “shockingly high” number of people have been regularly exposed to material causing them to question the safety of vaccines, said Imran Ahmed, chief executive of the Centre for Countering Digital Hate (CCDH), which monitors antivax content closely.
Oh this lot again.
[Wakefield] has used his Autism Media Channel to make videos asserting a link between autism and the MMR vaccine.
Yeah, that’s kind of his thing, have you not been paying attention for the past 25 years?
In interviews, he has said that autism is an “epidemic”
How is this NOT an epidemic???
and predicts one in 32 children will have autism in the US by 2030.
Pretty sure his prediction for 2030 is higher than this.
Meanwhile, it is one in 30 NOW so how is he wrong?!
To his supporters, he sells “Andrew Wakefield was right” T-shirts for $20.
Oh dear god the horror. I guess we should also cancel M&S. After all they sell t-shirts online too!
“Parents searching for answers about illnesses that come down to the lottery of genetics and disease are quite often susceptible to answers where there is a villain,” Ahmed said. “Bad actors like Wakefield know that by giving people a form of false hope mingled with blame they can create further advocates for their lies.”
Yeah because parents are too stupid to notice when their child regresses after a vaccine. Need I remind the author that it was the parents of the children in the Lancet study who said their children regressed after the MMR?
Though his mainstream social media following is small, his influence comes through backing other antivax projects and other antivaxers promoting Wakefield’s films, the CCDH said.
Stop the press! This genius at the “Centre for Countering Digital Hate” has figured out how the internet works! If people like content online they share it and recommend it! Heck forget the internet, how about this is how real life works? I thought it was supposed to be me with the shitty social skills.
Those include Robert F Kennedy Jr, the nephew of the former US president John F Kennedy, and the American television producer Del Bigtree, who leads a Texas-based antivax group.
Yeah, we know who RFK, Jr. is.
The author does know that Vaxxed: From Cover Up to Catastrophe is also Bigtree’s film as he was a producer on it? Actually probably not. That would involve research.
The idea of ‘pandemics’ and ‘outbreaks’ is one of the most convenient and effective ways for a government to sell fear and make money for their corporate backers (via vaccination drives). Although this did happen before Covid-19, such with the 2009 H1N1 ‘pandemic’, after Covid-19 the media has focused more on viruses and ‘pandemics’ in general, with random scare stories about viruses being grist to the MSM mill. Over the past few weeks, the idea of a ‘measles pandemic’ has been heavily pushed in the UK media. This article will discuss three aspects of this phenomena: the narrative, the purpose and the reality.
Part 1: The Narrative
Back in around September/October 2022, I noticed there seemed to be several random articles in the mainstream media about the ‘low uptake’ on the MMR (measles, mumps, rubella) vaccine.
For example, this article in the Daily Mail:
More than a third of children have not had their life-saving MMR vaccine in parts of England, according to official stats which illustrate why health chiefs fear a measles resurgence.
This immediately raised a red flag in my mind and got me thinking they might attempt to create a ‘measles pandemic’ and that this was the first signs of a new campaign.
Now, this narrative is back.
How are they building up the notion of fear?
The media has been recently filled with stories like this:
[T]he capital could experience an outbreak of between 40,000 and 160,0000 [yes, that typo is in the article] cases, fresh analysis by the UKHSA suggests.
We all know how successful modelling was with Covid. That is, successful at selling fear, because it certainly wasn’t successful at predicting ‘Covid cases and deaths’ since all the data it came out with were massive overestimates.
The model pdf report says:
[T]he risk of widespread transmission of measles, leading to a measles epidemic across the UK is considered low.
After that caveat (not mentioned in the media) we get into some nice fear porn like this:
Hospitalisation rates vary by age but range from 20 to 40%.
20% of even the fittest and healthiest age groups would be hospitalised for measles? Who believes this nonsense?
There doesn’t seem to be much of a ‘model’ in the report, their argument seems to be the lower vaccination rate in London means that the R (remember R from Covid fear porn?) is approaching 1 and this means there could be an outbreak:
[U]sing the UKHSA model, the reproduction number in London is now close to or above 1 (R=1.6, R=1.4, R=0.91) and could therefore result in an outbreak of between 40,000 and 160,000 cases.
The R rate (that is, the rate at which a virus spreads in the community, if you don’t remember it from Covid, so 1 means every infected person infects 1 other person) is calculated purely from vaccination rates among 25 and under. So far yet, this is purely hypothetical as there is no mass measles outbreak.
As to why measles has been selected for the fear campaign?
A measles outbreak seems a nice, likely candidate for a new fear campaign for a number of reasons. There is a large amount of (untrue) propaganda that a high mortality rate from measles was only stopped with the introduction of a measles vaccine.
Because measles is also a childhood disease, this evokes fear in parents that their child will die of measles. This contrasts with previous fear campaigns Covid-19, which clearly was not dangerous to children, and monkeypox/mpox/whatever-it-is-now, which largely affected gay men who had promiscuous sex.
Part 2: The Purpose
What’s the purpose of all this?
One of the main purposes is to sell MMR vaccination. Many of these articles fearmongering about measles (such as this one) have a picture of MMR vaccine vials – essentially product placement. You might not think the market would be that big – after all only young children get measles vaccines, right? But there’s actually potentially a bigger market than just young children available.
In fact, as per the UK Government, a large proportion of the population is not ‘fully vaccinated’ against measles, mumps and rubella. Why is this? Because the UK government deems that you need two doses to be ‘fully vaccinated’. The MMR vaccine (at 1 year) was introduced in 1988, but a second dose of the MMR vaccine (between 3-4) was not introduced until 1996, meaning 8 years of people not considered ‘fully protected’ who second doses can be sold to. Then there’s the people whose parents refused to let them have the MMR vaccination due to Wakefield’s paper. This group is referred to in the government press release as possibly ‘not fully vaccinated‘.
And then there are adults who were children before MMR was introduced. Presumably, these adults received a 1 dose measles single vaccine. Perhaps they are hoping that the endless fear porn will cause more people to ask their GPs for MMR vaccines. Many of the media articles stress that you can ask your GP about MMR vaccines if you are unsure of your vaccination status, as does the government press release:
Parents should check their children are fully vaccinated with 2 MMR doses, which gives 99% life-long protection, by checking their red book or with their GP practice, which younger and older adults can also do. Anyone not up-to-date should make an appointment as soon as possible.
Another purpose is to demonise antivaxxers, and also to set up the narrative of blaming antivaxxers for any cases that occur (real or fabricated). We can see this in a recent article from the Daily Mail. Dr. Ahmad Malik, a British surgeon sceptical of the Covid jabs, recently interviewed Dr. Andrew Wakefield for his podcast. The Daily Mail immediately put out an article on Wakefield’s ‘misinformation’:
The disgraced ex-doctor and godfather of the anti-vax movement sparked fresh outrage today by claiming kids shouldn’t be given any jabs. Andrew Wakefield made the hugely controversial comments in a new podcast.
While you do get occasional hit pieces on Wakefield in the media, why this podcast was selected for instant hatred was most likely due to the timing of its release – late July 2023. Wakefield has done multiple interviews with different alt-media (e.g. Steve Kirsch, UI Network, CHD) over the past few years without that much comment. However the timing of the release of the Malik podcast allows the media to blend this into their ‘measles pandemic’ push:
Fellow orthopaedic surgeon Dr Roshana Mehdian noted that Dr Malik was registered with the General Medical Council, the body that regulates medics in the UK. She noted that it comes ‘amidst a measles outbreak in London’.
Wakefield is ‘irresponsibly spreading’ ‘anti-vax disinformation’ ‘in the middle of an outbreak’ – where have we heard this tune before? This is a ‘measles outbreak’ that according to the article itself, consists of…85 cases.
The final function I will discuss is fear. That is pretty simple, to keep people in a state of fear so that if the government wants to revive policies like lockdowns in the future they will have an easier time of it. It has been demonstrated that people are more primed to accept authoritarian governments if there is a pandemic or illusion of a pandemic.
Part 3: The Problem
What do I mean by the problem? Vaccine failure. If we do get a resurgence of measles (which of course, is possible, although there is no evidence that this has occurred so far) vaccine failure will be the prime culprit.
The reality is that Measles/MMR vaccination has been a failure. The problem with vaccination is simple: while it is true that vaccination ‘produces antibodies’ the problem is that the manipulated solution of vaccination does not produce antibodies comparable to natural infection. This means that real immunity is not created to measles.
In short, levels of antibodies to measles are much lower since vaccination than they were prior to vaccination:
The study also found that adding a booster dose of the MMR vaccine only raises antibody levels in the very short term.
It’s also important to point out that all vaccination can do is put antibodies in the blood (regardless of the actual clinical meaning of those antibodies – as antivaxxers correctly argue, generating a bunch of antibodies is not proof of correlate of protection). The complex nature of the immune system is something not considered in vaccination (as discussed previously in this article). The complex responses created by natural infection are not something crudely rigging the immune system with vaccination can achieve. So if vaccination is even a failure at generation of blood antibody titers it’s a total failure.
James Lyons-Weiler also provided a helpful list of studies relating to measles vaccine failure on his substack. These are studies completed by vaccine promoters that nevertheless show real issues with measles vaccination. I cannot discuss all 25 (and of course, some of them are paywalled) but a glance at a few is worth our time.
One article from 1987 highlights vaccination failure was known even at that time:
An outbreak of measles occurred in a high school with a documented vaccination level of 98 per cent. Nineteen (70 per cent) of the cases were students who had histories of measles vaccination at 12 months of age or older and are therefore considered vaccine failures.
One of the articles highlighted by Lyons-Weiler is co-written by Greg Poland, one of the most fanatical vaccinators on the planet. This is the guy who got tinnitus from the Covid ‘vaccine’, acknowledges he got tinnitus from the Covid ‘vaccine’ and still took a booster. So if even this guy is acknowledging limitations of measles vaccination, we must be looking at some degree of failure.
Receiving less attention, however, is the issue of vaccine failure. […][W]e and others have demonstrated that the immune response to measles vaccine varies substantially in actual field use. Multiple studies demonstrate that 2–10% of those immunized with two doses of measles vaccine fail to develop protective antibody levels, and that immunity can wane over time and result in infection (so-called secondary vaccine failure) when the individual is exposed to measles. For example, during the 1989–1991 U.S. measles outbreaks 20–40% of the individuals affected had been previously immunized with one to two doses of vaccine.
For clarity we are talking about pretty small outbreaks here, so this as of yet cannot be taken as proof of mass vaccine failure. Nevertheless it demonstrates significant problems with the vaccine:
However, even with two documented doses of measles vaccine, our laboratory demonstrated that 8.9% of 763 healthy children immunized a mean of 7.4 years earlier, lacked protective levels of circulating measles-specific neutralizing antibodies [11], suggesting that even two doses of the current vaccine may be insufficient at the population level.
Meanwhile, the idea of measles ‘elimination’ via vaccination is a nonsense that is impossible, even with a mostly effective vaccine:
…measles eradication is unlikely as population immunity of 96–98% is required to prevent persisting measles endemicity [7,8,27,201]. In a recent study of measles-vaccine efficacy from 1960 to 2010, median efficacy was only 94% [28].
The UK government, media and establishment in general are attempting to push a fear based narrative around measles in order to sell MMR vaccination to the public and blame antivaxxers for any outbreaks. In reality, vaccine failure has been a contributing factor to outbreaks, and will continue to be so into the future.
The MMR (Measles, Mumps, Rubella) vaccine has been subject to controversy in the United Kingdom and worldwide, due to the 1998 Lancet paper by Wakefield et al. However there is one scandal around this vaccine that has been largely forgotten, despite the fact it has affected hundreds of thousands of UK citizens who were born in the late 1980s-early 1990s. This is the story of the MMR vaccines which contained the Urabe strain of mumps – and had to be removed from the Canadian, Japanese and UK markets due to causing aseptic meningitis in certain children. This episode demonstrates the corruption of the vaccine industry and the regulatory authorities in the United Kingdom in particular and shows that the deliberate use and promotion of known unsafe vaccines did not begin with Covid-19.
The History of the MMR Vaccine
Vaccination for measles, mumps and rubella was originally introduced in the 1960s. These were originally introduced as separate doses and not as a combined vaccine. For example, the measles vaccine was originally introduced in 1963 in the United States and the mumps vaccine was introduced in the US in 1967. The combined MMR vaccine was introduced in the 1970s in the United States and Canada, but somewhat later in some other countries, and in the UK in 1988. The MMR is a live virus vaccine, so it contains versions of these three different viruses that have been attenuated via running them through cycles in tissues in a lab.
However the virus strains in the MMR vaccine have not always been the same. There are multiple different MMR vaccinations that have been used since the 1970s, and one of the key differences has been the strain of virus employed to attempt to create artificial immunity. For example, a current vaccine in use, Priorix, contains the following strains of virus:
Though there have been differing strains of measles and rubella employed, this article is concerned with the mumps strains employed in the vaccines. According to a 1994 US government report on vaccine adverse events, there are three main strains of mumps used in MMR vaccinations: Jeryl Lynn, Leningrad-3-Parkow, and Urabe AM9. There have been differing vaccines using these strains, for example, both Priorix and MMR II use the Jeryl Lynn strain of mumps. There have also been multiple MMR vaccinations using the Urabe AM9 strain; the main two of concern in this article are Trivirix/Pluserix (two names for the same vaccine – the former used in Canada, the latter elsewhere) and Immravax. Although there is evidence that other strains of mumps virus used in MMR can cause aseptic meningitis as well, the Urabe strain has a significantly higher risk of this than the Jeryl Lynn strain based on the clinical data.
The Introduction of Urabe Strain MMR & Adverse Events
Although Canada used the MMR vaccine previously, the Urabe strain MMR was first introduced in Canada in 1986. In the UK, the MMR vaccine was introduced for the first time in 1988, and two out of the three vaccines that were used contained the Urabe strain mumps. Japan introduced these vaccines in 1989.
One significant side effect of these vaccinations was aseptic meningitis:
Aseptic meningitis refers to inflammation of the meninges [area surrounding brain and spinal cord], not of the brain. It can result from a variety of infectious, toxic, chemical, or physical agents. No bacterial organism can be identified in or isolated from the cerebrospinal fluid, but serologic studies often implicate a viral etiology.
It is possible for long-term harm to result, however, many cases resolve without long-term sequelae.
This section will discuss the evidence in detail for the conclusion that specifically the Urabe strain mumps component in these MMR vaccines causes aseptic meningitis. I will discuss multiple case reports and studies on this topic from medical journals in order to demonstrate the large amount of evidence that this vaccine causes aseptic meningitis and I will discuss the different article in the medical literature, in age order, starting with the earliest first. I will look at full articles when available and also abstracts where full articles are paywalled.
An early case report from Canada (dating from 1986, published in the medical literature 1988) reports a 14-year-old girl developing aseptic meningitis from a Urabe strain vaccine:
In October 1986 a 14-year-old girl with no history of measles-mumps-rubella vaccination was given Trivirix vaccine […] 26 days later […] she had clinical signs of aseptic meningitis.
Another Canadian source, an article published in the Pediatric Infectious Disease Journal in 1989, has the following to say:
All cases of mumps meningoencephalitis diagnosed at our institution during the past 15 years were reviewed. There were […] 5 [cases] in 1986 to 1988. Four of the recent cases occurred 19 to 26 days after receipt of a new mumps vaccine (Urabe Am 9 strain) released in Canada in 1986.
There is no other information provided in the abstract about the course of illness in the 4 cases. The US 1994 government document mentioned above discussing the study states than none of the 4 children had sequelae in this study.
An article from the British Medical Journal, 1989, discusses another proven case of aseptic meningitis after Pluserix:
[W]e also hesitated before reporting a girl aged 3 years and 2 months who developed proved mumps meningitis 21 days after being given mumps, measles, and rubella immunisation (Pluserix). […] The mumps virus isolated from her cerebrospinal fluid was identical with the Urabe vaccine strain used in her immunisation.
Another case report from the British context was published in the Lancet:
In 1989, Gray and Burns published two letters (Gray and Burns, 1989a,b) in The Lancet concerning a 3-year-old girl presenting with aseptic meningitis 21 days after vaccination with MMR. Fluorescent-antibody tests identified the isolated virus as mumps virus (Gray and Burns, 1989a), and soon thereafter, this virus was identified by nucleotide sequencing analysis as the Urabe strain (Gray and Burns, 1989b).
A 1991 article discusses Japan, where the Urabe vaccine was introduced in 1989. Japan had exactly the same issues with this vaccination as the UK and Canada:
Thirty-five children developed meningitis within 2 months after MMR vaccination during the 8-month period extending from April to November, 1989. The time lag between MMR vaccination and meningitis ranged from 14 to 28 days in the 35 cases of meningitis. The incidence of aseptic meningitis with positive mumps vaccine virus was estimated to be 0.11% (0.3% as a whole) during the 8 months from April to November and increased to 0.3% (0.7% as a whole) in September and October. We conclude that the incidence of aseptic meningitis after MMR vaccination seems to be higher than that reported previously.
Another article looking at Japan, again from 1991:
Among 630,157 recipients of measles-mumps-rubella trivalent (MMR) vaccine containing the Urabe Am9 mumps vaccine, there were at least 311 meningitis cases suspected to be vaccine-related. Meningitis was generally mild and there were no sequelae from the illness. The complication was more frequent among male than among female children.
For reference, the rate of Urabe strain mumps MMR vaccine meningitis would work out at about 1 in 2000 from this study.
A 1993 letter to the editor of the Archives of Disease in Childhood discusses underreporting of this vaccine complication:
Vaccine associated mumps meningitis was one of the conditions reportable to the British Paediatric Surveillance Unit (BPSU) between February 1990 and January 1992. During this two year period, 15 confirmed cases were reported. […] Based on the BPSU study the estimated risk of vaccine associated mumps meningitis in this age group was 1.5 per 100 000 vaccinations given. However when the BPSU data were supplemented by laboratory reports, a much higher rate of approximately 10 per 100 000 vaccinations was observed.
A 1996 article, this time from France, sought to retroactively assess the risk of this vaccination:
Fifty-four cases of AM were reported to the regional drug surveillance centres or to the manufacturer from the time each vaccine was launched up until June 1992. Twenty cases were associated with the time off administration of a monovalent mumps vaccine and 34 with a trivalent measles, mumps and rubella vaccine (MMR).[…] The global incidence of mumps vaccine-associated AM was 0.82/100,000 doses, which is significantly lower than the incidence in the unvaccinated population.
The rate was lower for the other MMR vaccinations.
A 1999 article acknowledges:
Aseptic meningitis is a well documented adverse event (1-4) that is attributable to the Urabe mumps strain of the combined measles-mumps-rubella (MMR) vaccine.
There was a mass vaccination campaign in Salvador, Brazil with the Urabe strain MMR vaccine Pluserix. The vaccination campaign en masse injected children from 1-11 within a very short period of time, just a couple of weeks. There was a significant spike in aseptic meningitis 3 weeks after ‘Vaccination Day’, providing further evidence of the dangers of this vaccine:
We conservatively estimated the risk of aseptic meningitis to be 1 in 14,000 doses (32 cases out of 452,344 applied doses).
A 2007 article attempts to assess the risk of aseptic meningitis with the Jeryl Lynn strain vis-a-vis the Urabe strain. It states that of 6 cases identified in computerised records between Jan 1991-Sep 1992, 4 were most likely triggered by a Urabe strain MMR vaccine. It further observes that the rate of aseptic meningitis from these vaccines can be estimated at about 1/12,500, and that:
The real risk of acute neurologic consequences from the Urabe mumps component of MMR was underestimated when using case ascertainment methods that were reliant on laboratory investigations
As we can see from the above evidence, there are a multitude of different estimates of the rate of Urabe strain-induced vaccine meningitis. The Japanese articles give the highest estimates, with 16.6/10,000 [1 in ~602] and 311/630,157 [1 in ~2000]. Surveillance was more intense in the Japanese context, with the 1996 study that gives us 16.6/10000 being based on active surveillance. This means the study authors are actively looking for the adverse event, rather than passive surveillance where something only gets flagged up when it happens to be reported by a doctor or patient (such as VAERS or Yellow Card). This will lead to a higher number of cases reported.
Other articles originating in other countries give a lower estimate of aseptic meningitis. These articles seem to be based on retroactive studies of hospital admissions for aseptic meningitis and may be less complete than studies based upon active surveillance. Nevertheless they still give a rate of around 1 in 14,000-1 in 10,000.
However all these articles are agreed in either the suspicion or the fact that the Urabe strain MMR does cause aseptic meningitis. In many cases discussed the Urabe strain mumps was found in patient samples. In other words there is no real debate about this: the vaccine causes aseptic meningitis. I could not find a single article dissenting from the view that the vaccine is responsible for at least some observed cases of aseptic meningitis.
Political and Medical Corruption Behind the Urabe MMR Vaccine
We are immunising the children and the government is immunising us.
SmithKline Representative to MMR whistleblower, as reported to Andrew Wakefield (Callous Disregard, p. 68)
This section will focus on the UK situation only, and not upon the introduction and use of this vaccine in other countries.
Let’s start with the Guidelines for the MMR vaccination, published in the British Medical Journal in 1988 [the vaccine was introduced in October of that year]:
The vaccine will be available from two manufacturers, Smith Kline and French [Trivirix/Pluserix] and Merieux UK [Immravax]; both vaccines contain the same strains of virus: Mumps; Urabe AMI9. This has been in use in the Smith Kline and French vaccine in Europe and Asia for three to four years.
Measles, mumps, and rubella vaccine: The following guidelines on the use of the measles, mumps, and rubella vaccine have been sent by the Department of Health to all general practitioners.
The comment relating to the Urabe strain is clearly meant to imply that it is safe for use, since if if has been in use for 3-4 years, that makes it safe, right? Interestingly, there is no comment in this document regarding the strain of measles or rubella, indicating a defensiveness about the mumps vaccine strain in use.
The ‘Adverse reactions’ section says the following (in full):
As with measles vaccine, malaise, fever and/or a rash may occur, most commonly about a week after vaccination and lasting about two to three days. Parotid swelling [glands near the jaw] occasionally occurs, usually in the third week; children with postvaccination symptoms are not infectious. Parents will be given information and advice for reducing fever, including the use of paracetamol in the period 5-10 days after vaccination. Serious reactions should be reported to the Committee on Safety of Medicines using the yellow card system.
As we can see, there is no reference to the possibility of aseptic meningitis in this section. However, as we can see from the above literature, the possibility of aseptic meningitis had already been raised as an issue in the Canadian context, with cases of aseptic meningitis having been reported very soon after the vaccine’s introduction, with the two articles above from Canada highlighting some of these cases.
However it gets worse. Not only were there cases in Canada, but:
Pluserix had been licensed in numerous countries prior to 1988 but unbeknown to the British public, far from it having a good record in these countries, the vaccine had already been withdrawn in Canada, where it had been marketed as Trivirix, following the discovery of adverse reactions of aseptic meningitis. [original emphasis]
The Canadian Chief Medical Officer of the Ontario Ministry of Health stated all of these vaccines had to be sent back and no longer used in July 1988. Canada eventually went further and pulled the license of the vaccine in 1990.
The UK decided, essentially, to ignore the Canadian experience with these vaccines and introduce them anyway in 1988. When assessing the safety of the MMR vaccine, they used irrelevant data from countries using a completely different MMR vaccination, such as the US. This data was accepted as relevant despite the differences in the vaccinations. They rushed through a license for the Pluserix vaccine, in order that their announced MMR program could go forward as per schedule. Furthermore, the whistleblower mentioned at the top of this section, who had worked in the Canadian system and seen the harms of the vaccine, advised the JCVI that it should not be used, but he was ignored by more senior members.
As mentioned in the header, it appears the company SmithKline had no liability for these vaccinations and adverse events caused by them. Instead the government seemed to be the party liable. This situation continued; the JCVI minutes in 1993 state that the manufacturers “continue to sell the Urabe MMR without liability” (cited in Callous Disregard, p. 74). The UK stopped using the vaccines in 1992, but did not pull the license which helped to enable the use of the vaccine in other countries (such as Brazil in 1997 – see above cited article). This meant injuries caused by these vaccines continued to occur.
What can we conclude? The main concern of the UK authorities was not to ensure the safety of the vaccine, but to ensure the political success of the MMR program.
There are very powerful people in positions of great authority who have staked their reputations on the safety of MMR and they are willing to do almost anything to protect themselves.
The success of a vaccination program, as defined by the establishment, has nothing to do with the safety or effectiveness of a vaccine. Instead, it is purely a political and religious construct about getting needles in arms. The corruption in vaccination programs is not a new development with the ‘Covid-19 pandemic’, instead it has existed in previous vaccine campaigns.
Appendix: Personal Comments on Urabe Strain Mumps MMR.
I received the MMR vaccine in 1989. At the time, 85-90% (different sources give slightly different figures) of the MMR vaccinations in use in the UK contained the Urabe strain mumps. As aseptic meningitis is a specific form of inflammation around the brain, it is not far fetched to suggest a possible link to autism (given that autism is an inflammatory disease) – although as far as I’m aware there has been no direct evidence regarding this question. Of course, the US, with its skyrocketing rates of autism never used these specific vaccines, and MMR vaccination is not the only factor to consider in autism.
With this in mind, I tried to find out specifically which MMR vaccination I received, so I wrote to my GP surgery and asked for the ‘brand and/or batch/lot’ of MMR vaccine I received. They sent me my vaccination records, which appears to not contain this information, so I was not able to confirm whether I received a Urabe-containing vaccine. However, I did receive a message from the GP surgery on my letter enclosed with the vaccination records that the surgery is a “Vaccine Positive practice” that “Vaccination is one of the greatest success stories in modern medicine” and that it “saves lives and prevents suffering.” Bear in mind, the only question I asked was about the brand and batch/lot of MMR vaccine I received: I made no reference to adverse events in any way. Apparently even asking about this basic information is too much of a question for the vaccination cult.
Robert F. Kennedy, Jr. is currently serving as an important hate figure for the mainstream media and establishment, due to his run for US President and his opposition to the mRNA/adenovirus vector covid ‘vaccines’ and scepticism of the CDC childhood vaccination schedule. In particular, his belief that vaccines cause autism is unacceptable to the establishment. That establishment, a fundamental pillar of which is the vaccine cult, finds the idea of truths stated by RFK, Jr. about vaccines becoming more widespread impossible to countenance. However the establishment has a huge problem: they have overplayed their hand with Covid by pushing such a deadly, obviously unsafe, and obviously ineffective product. This has caused many previously pro-vaccine people to be open to ideas such as ‘vaccines cause autism’ in a way that simply wasn’t the case before 2020. The establishment has now gone into defensive mode to protect the vaccine cult, as the idea that vaccines cause autism, and thus have completely destroyed lives, is something the establishment cannot admit because it will be a very big blow (possibly fatal, we can live in hope) to the vaccine paradigm.
As such, the establishment needs as many hit pieces on RFK, Jr. as they can muster. The latest anti-RFK, Jr. article is out, written by Matthew Rozsa, an autistic man very fond of the neurodiversity paradigm, claiming that RFK, Jr. hates autistic people.
I have posted a couple of responses to him on Twitter, pointing out the reality of those who are severely impaired by autism, but so far have been ignored.
So let’s break the article down. As usual, the only way I will be able to deal with such weapons-grade bullshit is by chucking some sarcasm in there. For those who happen to be new to this page, I have an autism diagnosis so I have personal experience of the lies this guy is trying to sell.
Let’s start with the subheading:
RFK Jr. says he advocates for the marginalized, but built his career spreading harmful lies about autistic people
Kennedy hasn’t ‘built his career’ talking about the issue of vaccines and autism, since this ignores all of Kennedy’s environmental work before he got into the vaccine issue and realised that mercury in vaccines was causing harm alongside the mercury in the air and water.
[E]xperts agree on one thing: The views that RFK Jr. espouses cause significant harm to real-life autistic individuals.
As opposed to what? Non-real life fake autistic individuals?
I haven’t been harmed in any way by Kennedy or anything he has said.
Autistic people have been victimized by RFK Jr. for decades.
‘Victimized for decades’. Because he agrees that vaccines cause autism. Get a grip, honestly, if you are that sensitive.
RFK Jr. has never retracted his views or apologized for his incorrect statement that thimerosal in childhood vaccines can be linked to a rise in autism.
Because there is no reason to retract them. Mercury is toxic and causes harm to the brain. This is proven. That there is some sort of ‘good’ mercury that doesn’t harm the brain is provaxxer nonsense.
Quite to the contrary, he has started applying his formula of “use bad science to persecute marginalized groups” in brand new ways, such as falsely stating that the rise in “sexual dysphoria” is caused by “chemical exposures” despite there being extensively documented historical andscientificvalidation of transgender identities.
Oh we have got to get at least one reference to ‘trans women are the most marginalised people on the planet’ have we?
The so-called ‘historical’ validation of ‘transgenderism’ usually amounts to pointing to societies that had special categorisations for same-sex attracted males that classified them as some third group (and not as male). They were not considered to be actual women. The implication that these ‘third genders’ were in some way politically progressive – when they are based on homophobia and misogyny – is also false. The other argument for ‘historical’ validation of ‘transgenderism’ I have seen used is claiming that women who disguised themselves as men due to sexism to access certain positions were actually ‘transgender’, or women who had a stereotypically male role, such as Joan of Arc, were actually ‘transgender’. This is obviously regressive nonsense based on stereotypes and just a way to claim a historical lineage for modern ideas.
Also, as argued by 4thWaveNow, the phenomena of ‘trans kids’ who will die if not ‘affirmed’ has no historical basis:
Try as I might, I was unable to discover any evidence of ancient trans kids who so hated their own bodies that they demanded either psychological or medical interventions. No records of boys wanting to hack off their penises or girls desperate for “top surgery” to remove their despised breasts. It’s quite certain, given their zeal for surgical interventions, that the ancient physicians [in Greece and Rome] would have been more than happy to oblige; after all, if they could perform surgeries to treat urethral strictures and cataracts, a double mastectomy or penile remodeling would not have daunted them. Even experimental attempts would have been documented.
The ‘scientific’ validation studies are generally brain scans, claiming that men who call themselves women have more similar brains to women than men. However these studies often don’t control for homosexual attraction and if a man has already taken female hormones that will affect his brain. Of course a male having a stereotypically ‘feminine’ brain (if such a thing even exists) doesn’t make him a woman since every cell in that brain is a male cell with XY chromosomes, etc.
On the other hand, Kennedy’s assertion that certain chemicals could cause gender dysphoria, or contribute to it, is scientifically plausible. We know that phthalates mimic estrogen, for example. That this mimicking could be a factor affecting gender dysphoria in boys or men is certainly possible. I think there is a large social/monetary aspect to this, so I don’t think endocrine disruptors are the only cause of the ‘transgender’ insanity we see today. However that they could contribute is plausible (even the article linked by the writer claims that Kennedy ‘in part’ blamed chemical exposures).
Furthermore, do you care to comment on the obscenely high amount of autistic people going in for ‘gender transition’? In fact, being as you think that autism is genetic and the fact that ‘gender’ treatments like puberty blockers followed by wrong sex hormones sterilise children, shouldn’t you be calling this eugenics?
It is very common for autistic people to encounter anti-vaxxers who claim that their neurology is somehow a mistake. Because they buy into the perennial RFK Jr. assertion that vaccines cause autism and other neurological disorders, they make the next logical leap that another person’s autism is “wrong.”
Of course it is ‘wrong’. It’s a disability, therefore it involves inferior functioning in some way. That’s what the word ‘disability’ means. The implication here is that calling autism ‘wrong’ is some sort of moral judgement on the vaccine-injured person but that is not the case.
Even if this attitude is intended sympathetically rather than contemptuously (which is definitely not always the case), the anti-vaxxer logic still causes neurotypicals to ablesplain about how autism really works — or to outright discriminate against them.
You are assuming that there are two groups, neurodiversity promoting autists and ‘neurotypical’ antivaxxers. But autistic people can also be antivaxxers. I know I am one. We can also recognise that our problems come from vaccines. I do.
So do you want my back-of-a-fag-packet explanation of autism?: Autism is a form of iatrogenically induced brain/gastroenterological inflammation, in most cases created by the toxicants in vaccination such as aluminium.
Many autistic people have a dim view of RFK Jr. for that reason.
I don’t.
Steve Silberman, author of the book of “NeuroTribes: The Legacy of Autism and the Future of Neurodiversity,”
Who isn’t an autist and knows nothing about the misery of autism. I thought you didn’t want non-disabled people explaining autism to disabled people. Or is it ok if the non-disabled person wants to glamourise autism for money/clout/woke points?
Silberman ticked off two of the most infamous examples: RFK Jr. regularly using the term “vaccine-injured” to refer to autistic people
Because we are vaccine-injured. Honestly why are people so offended by this? If I refer to someone who lost a leg in a car crash as car-crash-injured no-one is going to give a shit.
and in 2015 describing vaccinated autistic children to Bill Maher by saying “their brain is gone.”
Maybe not the best turn of phrase but you know damn well what he means. You know damn well he is referring to those children who were developing normally, were given vaccine/s and horrifically regressed, lost speech, lost eye contact, lost the capacity to use toilet alone, starting having seizures, had severe gastrointestinal issues, etc.
“Grotesque statements like this present people on the spectrum as entirely lacking in humanity, agency and the potential for development — as if they were zombies,” Silberman explained.
Nothing Kennedy has said has even implied autistic people are not human. That is a lie.
As for ‘agency’ and ‘potential for development’ well it really depends on the severity of the vaccine injury. The reality is that severely autistic people have very little agency or potential for development. If someone is so severely impaired they need 24/7 care what agency and potential do they have? You can call this statement ‘ableism’ till you’re blue in the face but it’s just fact. Of course, that may change if they receive treatment for their vaccine injuries and recover some capacities destroyed by vaccines, but you are against treatment for autism so what else do you suggest?
“He compares autistic people to Holocaust victims, which does a grave injustice to both autistic people and Jews. And even in apologizing for that comparison, he described autism as ‘shattering’ families, when some of the most loving and supportive families I know are the families of autistic people.”
Silberman isn’t the mother of those children so he can walk away at any time. I have no doubt some of these parents are genuinely supportive but he needs to try and consider the reality of caring for a severely impaired child 24/7/365. For example, they may require 24 hour supervision, cannot use the toilet alone, can have seizures (which includes risk of death). Furthermore they grow up. Imagine you are a 5′ 5″ mother attempting to subdue your severely ill, autistic, 6′, 20-year-old son when he is lashing out in a fit of violent rage due to sensory overload and then get back to me.
It is also true that the strain of severe autism on a family can lead to divorce, the severely disabled child requires all the attention 24/7 so siblings are neglected, etc. Again, this is fantasyland stuff from Silberman.
“The main problem that autistic people and their families face is the lack of support and resources across the life span, but Kennedy condemns the ‘crippling’ cost of providing disabled students with access to education, using an ableist slur to complain about resources that were fought-for by generations of disabled people and their families,” Silberman pointed out.
So this man, who isn’t autistic, is telling autistic people what our ‘main problem’ in life is. While this article preaches about ‘non-disabled people explaining autism to autistics’. Yeah piss off.
‘Crippling cost’ of so and so is a pretty stock phrase. Neurodiversity activists want to have this both ways. They want to claim autism is a disability when they want accommodations or money but then want to glamourise & claim it’s just a ‘difference’ and does not imply inferior functioning. These two claims contradict each other. Pick one.
“It increases vaccine hesitancy and people choosing not to give their kids vaccines, and that increases the resurgence of vaccine preventable diseases,” Zoe Gross, director of Advocacy at the Autistic Self-Advocacy Network, told Salon. Perhaps the most prominent instance of this occurred in 2015, when nearly 200 people were sickened with measles despite the disease having been eradicated 15 years earlier due to parents not vaccinating their children.
Yes the point of vaccine scepticism is to try and get people to not give their children poison injections, well done for figuring that out.
I said this with Covid and I’ll say it again: ‘cases’ of a disease are irrelevant. If someone gets sick for a week with measles, so what? This nonsense that we can simply eradicate disease with the needle and we never have to be sick from anything ever is a ridiculous provaxxer fantasy.
“You can see that these are people who would rather have their kids get vaccine-preventable diseases and potentially die than do something that they think erroneously risks their kids becoming autistic. That’s a pretty bleak view of autism.”
Reality is a pretty bleak view of autism.
Life expectancy of 36-39.5 for the low functioning cases, 58 for the high functioning ones, 78% unemployment rate, misery of sensory issues, high anxiety, loneliness, non verbal, seizures, can’t use the toilet on their own, gastroenterological problems…yeah why would a parent not want that for their child? If you’re offended by this, you’re offended by reality. Feel free to go off in the corner and be offended by reality but the rest of us don’t have to take you seriously.
As a result, Waltz described how in the 1990s the “‘do your own research’ crowd” created a climate wherein “autistic children were written off by most schools and psychologists, parents were left without the services they and their children needed, and autistic adults weren’t even in the conversation.”
Yeah the reason that autism got no funding was antivaxxers, because we all know that antivaxxers are all-powerful & control the reins of the government purse.
They also encouraged the view that autism is an “epidemic,” so that research goes toward “curing” it instead of things like “local charities and services that were helping children, families and adults, and diverted funds away from the research into education, social care, family support, housing and employment that would help actually existing autistic people and those who care about them.”
How is this not an epidemic? Please explain with a rational argument, and not ‘those mean antivaxxers said it’.
Again, antivaxxers aren’t the ones controlling the money. I know you all think we’ve all got mansions and shit but for the vast majority of us: no.
“His insistence that autism is a recent phenomenon caused by vaccines or chemical pollutants erases generations of autistic people who were often misdiagnosed with conditions like childhood schizophrenia, and subjected to cruel ‘treatments’ including lobotomies and brutal punishments for autistic behavior that included electric shocks,” Silberman observed.
Except those treatments were very late 19th/20th century (lobotomy) or became popular in the second half of the 19th century with origins in the 17th/18th century (electroshock), so they have been mostly used well into the vaccine & pollutant era. Schizophrenia is also quite a modern term, coined in 1900. In fact, like vaccines, these ideas are largely an invention of the modern Victorian medical paradigm. So this does not prove the long history of autism. You need to be proving the mass cases of regressive autism among peoples like the Greeks and the Romans to prove it’s normal (I say Greeks and Romans because they had good records so it would be possible to prove, but completely non-settled pre-agricultural societies where there would be little/no exposure to mercury would be best).
Furthermore, electroshock therapy is still used by psychiatry. Does Silberman consider that to be barbaric as well? I don’t have a problem condemning it, but it involves condemning the modern medical establishment and well, we can’t question ‘The Science’. We wouldn’t want to be considered ‘conspiracy theorists’ now would we?
“That’s precisely the opposite of the truth — in fact, study after study has shown that the broadening of the diagnostic criteria was instrumental in boosting estimates of autism prevalence, as I discuss at length in my book NeuroTribes.”
No-one is saying that this is completely irrelevant, but the idea of something going from 1 in 10000 to 1 in 36 just because of extra diagnostic criteria is absurd on its face.
But let’s just quote Toby Rogers:
Well perhaps the increase in autism prevalence is just the result of better awareness (and what’s called “diagnostic expansion and substitution”)? The state of California funded two multimillion dollar to examine sharply rising prevalence in the state and whether it was the result of social factors. The first study was led by pediatric epidemiologist Robert S. Byrd at UC Davis who directed a team of investigators at UC Davis and UCLA. The investigators concluded that, “The observed increase in autism cases cannot be explained by a loosening in the criteria used to make the diagnosis” and “children served by the State’s Regional Centers are largely native born and there has been no major migration of children into California that would explain the increase in autism” (Byrd et al., 2002).
The state of California revisited this question in 2009 with a study led by the top environmental epidemiologist in the state — Irva Hertz-Picciotto at the UC Davis Mind Institute. This study concluded that changes in diagnostic criteria, the inclusion of milder cases, and earlier age at diagnosis explain about a quarter to a third of the total increase in autism (Hertz-Picciotto & Delwiche, 2009). In a subsequent interview with Scientific American, Hertz-Picciotto explained that these three factors “don’t get us close” to explaining the sharp rise in autism over that time period and she urged the scientific community to take a closer look at environmental factors (Cone, 2009).
The entire conspiracy theory that vaccines cause autism can be traced back to 1998, when a British doctor named Andrew Wakefield published a study in the medical journal The Lancet claiming that children who were given the measles, mumps and rubella vaccine (MMR vaccine) developed autism.
Oh goodie the obligatory Wakefield-bashing. Do they ever get tired of stating the same shit? Where would provaxxers be without Andy Wakefield to bash a few more times?
The Wakefield Gambit, as used by provaxxers, is something like this: Andrew Wakefield said that the MMR vaccine causes autism and he is a bad man and a fraud so therefore vaccines don’t cause autism. Despite obviously being fallacious, the main purpose of this argument is to erase other doctors or experts that have researched this topic (Dr. Exley, Dr. Thomas, Dr. Bradstreet, for example) by implying it’s only Dr. Wakefield who said it and then that if they can discredit him they can discredit the whole thing. Perversely this argument then ends up giving Andy Wakefield all the credit as the single handed destroyer of vaccine ‘science’ which is probably the opposite of what they want to achieve given how much they hate him.
Let’s address the actual argument. If I have said this once, I have said it a hundred times. The people who claimed that the children developed autism after the MMR vaccine were the parents of the children. Wakefield was simply willing to listen rather than automatically gaslight the parents. Read the goddamned Lancet study.
Onset of behavioural symptoms was associated, by the parents, with measles, mumps, and rubella vaccination in eight of the 12 children
“That’s not the same as saying that autistic people and their families are always just fine,” Waltz clarified. “We’ve created a society that excludes more and more people from the norm, and we could do something about that by changing our attitudes and behaviors regarding human diversity. But of course there is also that one-quarter to one-third of the autistic population who also have intellectual disabilities, and there are those with very severe sensory perceptual issues or additional medical needs (for example, due to seizure disorders, which are more common in autistic people).”
Oh now you acknowledge those severely impaired by autism. Right at the bottom. Because they aren’t glamourous enough for ~neurodiversity~.
Also the framing on these things annoys me as it tries to minimise the problem of the autism, and makes the problem about ‘lack of acceptance’. No the problem is the damn autism. Funnily enough no-one’s expressed any real hate towards me for autism but that hasn’t managed to magically cure my severe anxiety and my sensory issues (fortunately I have managed to cure the severe anxiety with Dr. Chris Exley’s method) but the neurodiversity activists pretend that if people are nice to me I would have little or no problem. That’s without even mentioning severe autism.
These individuals need help in the form of social services. What they definitely don’t need, Waltz said, is “to be someone’s ‘experiment of one’ to be put through potentially harmful therapies and treatments, not someone to be over-medicated for behavior control rather than medical need, not someone to be institutionalized or abused.”
Where has Kennedy suggested ‘over-medicating’ autistic children? I’m guessing given Kennedy’s stance on Pharma, he’d be opposed. Isn’t it the establishment who think drugs for every ‘mental health’ problem are good and that if you object you are ‘pill shaming’? This article is meant to be criticising Kennedy and well if it isn’t a claim Kennedy has made I don’t see the relevance.
Image source: Photo by Mateus Henrique on Pexels.com
Vaccination is considered by mainstream society to be a scientific practice, with no other motivations behind it other than those based in evidence. However, vaccination is not actually a scientific practice, but a cult practice, and this article will outline the reasons why vaccination can fundamentally be considered a cult.
I. The Promise of Salvation
All cults begin with the promise of salvation. The promise of salvation in the vaccination cult is the eradication of that we most fear: disease and death.
Death is humanity’s biggest fear, broadly speaking. It’s fair to say that this applies to most human beings, although there are exceptions to this rule. Disease and illness is also another large fear, that we will become ill and will be unable to care for ourselves and our families.
Vaccination offers to remove all our fears and doubts about death and disease. It offers what I would call the ‘Fantastical Conquest of Disease Narrative’, as a means to eliminate this fear. This narrative goes something like this:
In the time period Before Vaccination, people were constantly dying of disease. There were deadly outbreaks of diseases like smallpox which killed millions. Then Edward Jenner invented to concept of inoculation via cowpox, and soon the Smallpox Vaccine would come to save millions of lives. As the Industrial Revolution progressed, and science developed more and more, more and more life saving vaccines were developed. Because of this, disease plummeted. Vaccination is the reason that we have a good quality of life today and don’t have to worry about our children dying from measles, etc. Now, After Vaccination, we have our salvation.
II. The Receipt of the Salvation Ritual
However, in order to gain salvation, one must submit oneself or one’s children to the receipt of the Baptism of the Injection.
The receipt of the injection is a cult ritual. It is a sacred act. One is prepared for the receipt of the injection by the doctor, the modern day priest. The clean sterile environment, free of danger, germs, serves like the stained glass of old – to induce reverence, and as a reminder of what bounty one (or one’s child) will receive for undergoing the pain of the needle – a sterile, germ free body. Like the priest, the doctor reassures, soothes, it will all be over soon like an awkward session of confession. It is to save one’s body like confession is to save one’s soul. Sleeves are rolled up, skin prepared, pricked, plungers pushed. Maybe the child cries: he does not understand this is to save him. The doctor puts a plaster on it. There, all done, all over, the ritual is completed. There are lollipops, see, to soothe the pain.
To inject one’s children with vaccines is to induct them into the cult of vaccination, and this is the societal function of paediatric medicine. The whole function of institutions such as baby check ups is to establish compliance with the cult rituals of vaccination and ensure all doubt is removed from the parents’ mind. The indoctrination of the broader society into the narrative that vaccination is always good, via the media and government, is pervasive, but there may still be some parents who have questions. Perhaps something broke through to them on a social media platform, perhaps they heard another parent talk about suspected vaccine injury in their child. Doubts cannot be allowed to fester, they must be smoothed over with the concrete of authority to fill in the cracks. You see, the doctor knows best.
The Covid-19 Narrative has allowed for even adults to themselves confess their faith in Vaccination via the Covid-19 ‘vaccine’ products. Prior to Covid, adult vaccinations were not all that important – even the flu shot, which is pushed to an extent, did not reach the sanctity of the childhood vaccination schedule. With Covid, adult vaccinations became fundamental. An adult must not only confirm their faith by injection of these products into their children, but receive them personally. And so many followed suit! Not only did they receive the holy ritual of vaccination, they openly expressed their reconfirmation of faith in vaccines on social media. How many selfies with ‘I’ve Had My Covid-19 Vaccine’ did you see? How many images of a masked, presumably smiling face, with a white-coat hovering over them pushing a plunger? The constant receipt of Covid ‘boosters’ – indicating the failure of the initial series, else why would ‘boosters’ be required – also serves as a reconfirmation of faith.
Vaccination also gives meaning to people’s lives. No doubt the quote above is an exaggeration – I’m sure there are atheists who question vaccination – it nevertheless makes an excellent point. The decline of traditional religion has meant that people do not have meaning in their lives, and even more so with the mass modern atomisation of traditional communities. Preaching the Gospel of Vaccination – like so many scientists, bureaucrats and general do-gooders do – provides a helpful alternative to create that meaning.
In general, those that are opposed to vaccination are seen in a negative light – and there are two categories of such people: The Hate Figure (more on hate figures below) and the Ignorant (who concern us here). The Ignorant are seen as needing education from the white-coat about vaccination, as being too stupid to understand, and they just need to accept the offer of salvation from the white-coat. In the Western internet age these people are often seen as dupes of evil, malicious hate figures – i.e. the main spokespeople of the anti-vaccination movement, who in a tremendous example of projection are only out for money.
There is also a large aspect of a White Saviour Complex to this narrative, with ‘ignorant’ Africans needing to be educated by white Westerners about vaccines, so that they can be ‘saved’ by the receipt of the injection. Any institutions that stand in the way of the delivery of more vaccinations in any African country – such as on occasion the Catholic Church – are demonised regardless of the truth of their claims or legitimacy of their questions about vaccination.
Any questions about vaccination are dismissed as ‘reactionary’, ‘right-wing’, ‘anti-science’ – these simply stand in the way of ‘progress’, progress defined as shiny tip of a needle.
IV. The Apostate as Hate Figure
One of the most notable features of a cult is that it cannot tolerate dissent, and must silence any critique. One method how this is done is the creation of a hate figure – a person who represents what the cult does not.
When it comes to the vaccination cult the most notable hate figure is Dr. Andrew Wakefield. The Official Narrative, repeated ad nauseam in the mainstream media, is that Wakefield is a disgraced, immoral fraud. The endless repetition of this narrative provides a hate figure for believers in the vaccine cult to pour their wrath upon. Like the Two Minutes Hate in 1984, this hatred reinforces the belief in the narrative. But the hate figure can also act as a balm for the reason why vaccination has not achieved its salvation promise of elimination of disease and death. We see this whenever there is an outbreak of measles or mumps anywhere. Because of Wakefield’s criticism of the MMR vaccine, he gets the blame. There was an outbreak ‘because disgraced British doctor Andrew Wakefield convinced parents with his lies not to vaccinate with the very safe MMR vaccine’, not because of any problems with the concept of vaccination or the vaccine program. The truth is irrelevant, the target is set, and any questioning of the cult is cut off.
And of course the most obvious reason for the creation of a hate figure is to inculcate fear – to make someone questioning the cult think twice about leaving, lest they be demonised and lose their career and income. This serves to keep any other doctor in line who might think about questioning vaccines. Fundamentally, Dr. Wakefield fits the role of cult apostate: he (and prior to him, members of his family) trained in the mainstream medical system – one of the pillars of which is the worship of vaccination. Thus his trial before the General Medical Council and by media, and his eventual striking from the medical register, should be seen through the lens of excommunication.
Conclusion
The four aspects outlined above serve as the basis for the establishment and maintenance of the vaccine cult in society.
I don’t usually put out short commentaries/news type posts as I generally like to keep the blog as a place for long posts or protest coverage. However in this case, this news story is so worthy of note, and I have seen very little on it out there so far, and I am so angry about it, that I am making an exception.
The media today in the United Kingdom have just reported the below story, headlined:
The 32-year-old, who can’t be named for legal reasons, spent lockdown in his room at a care home because his parents refused to let him be vaccinated, Jersey’s Royal Court heard.
To translate this from mainstream media bullshit to English, the care home locked him in his room because his parents did not want him to be harmed by a ‘vaccine’. When he had already been harmed by vaccines. His parents should have had him removed from the care home, if possible, although some of these care homes have put obstacles in the way of getting people out and I don’t know if that’s the case here.
Jersey’s Royal Court granted the vaccination order, saying that it was ‘the right best interests decision’ for B who had been in ‘groundhog day’.
In other words, this man is stuck because the care home won’t let him out because he’s not jabbed so they want to force him to be jabbed. When they could get rid of the problem by simply not treating him as subhuman for not being jabbed.
This also involves denying him treatments, according to the Times:
He is not able to attend the treatments, such as hydrotherapy, which soothe him, or the ones that cheer him, such as watching the Christmas lights being turned on, stuck in what his nurse describes as a “shrunken world”.

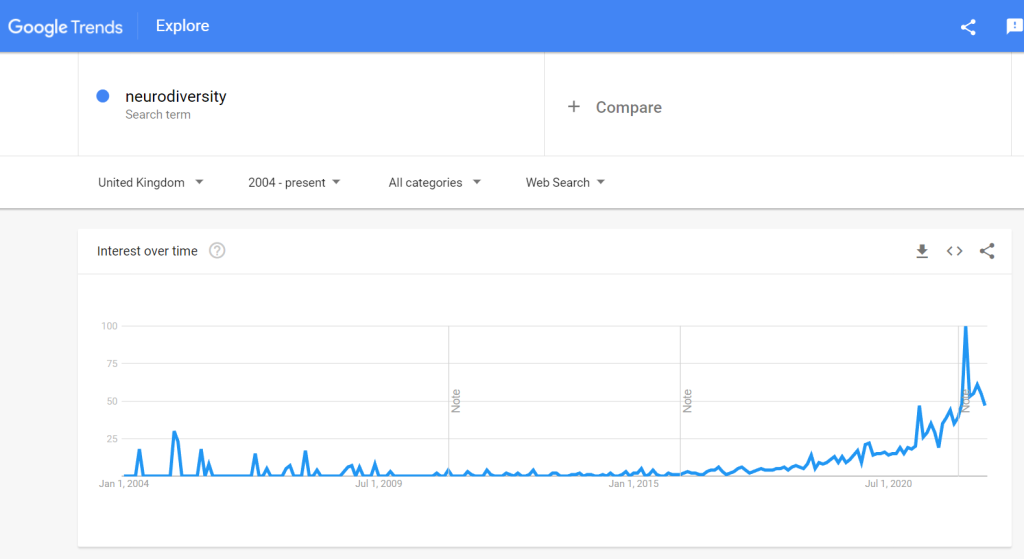
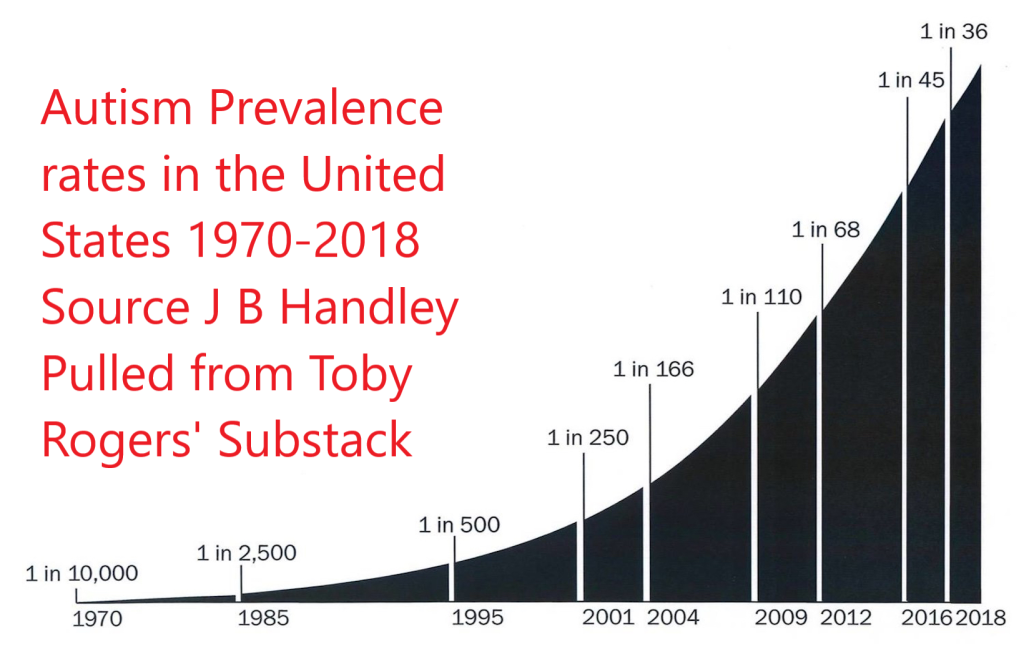



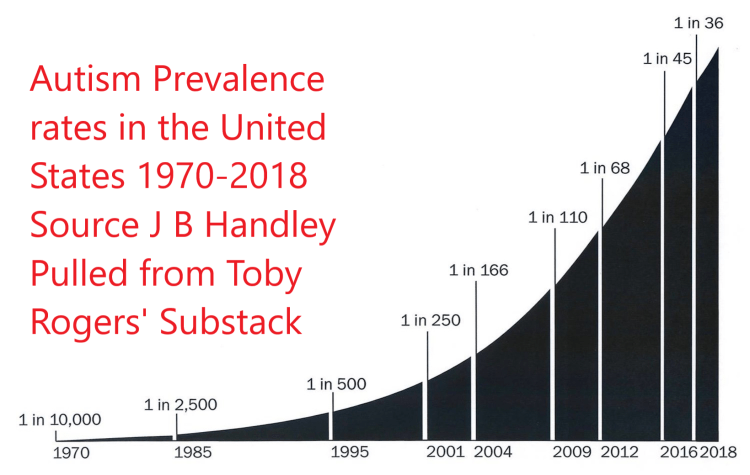

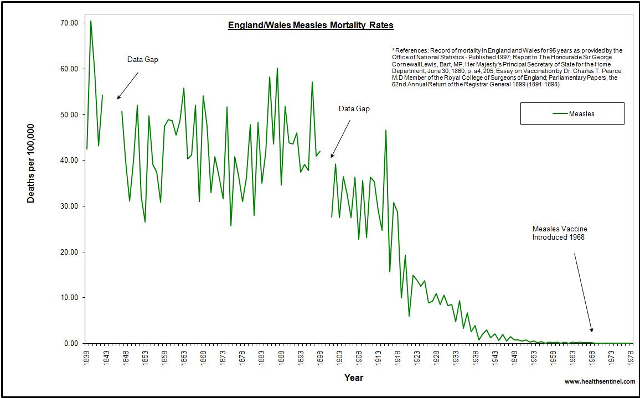







{kind=link}