“In the area of vaccination, since its inception, the public has paid a price for an illusory peace of mind.”
Martin J Walker MA
Introduction
The MMR (Measles, Mumps, Rubella) vaccine has been subject to controversy in the United Kingdom and worldwide, due to the 1998 Lancet paper by Wakefield et al. However there is one scandal around this vaccine that has been largely forgotten, despite the fact it has affected hundreds of thousands of UK citizens who were born in the late 1980s-early 1990s. This is the story of the MMR vaccines which contained the Urabe strain of mumps – and had to be removed from the Canadian, Japanese and UK markets due to causing aseptic meningitis in certain children. This episode demonstrates the corruption of the vaccine industry and the regulatory authorities in the United Kingdom in particular and shows that the deliberate use and promotion of known unsafe vaccines did not begin with Covid-19.
The History of the MMR Vaccine
Vaccination for measles, mumps and rubella was originally introduced in the 1960s. These were originally introduced as separate doses and not as a combined vaccine. For example, the measles vaccine was originally introduced in 1963 in the United States and the mumps vaccine was introduced in the US in 1967. The combined MMR vaccine was introduced in the 1970s in the United States and Canada, but somewhat later in some other countries, and in the UK in 1988. The MMR is a live virus vaccine, so it contains versions of these three different viruses that have been attenuated via running them through cycles in tissues in a lab.
However the virus strains in the MMR vaccine have not always been the same. There are multiple different MMR vaccinations that have been used since the 1970s, and one of the key differences has been the strain of virus employed to attempt to create artificial immunity. For example, a current vaccine in use, Priorix, contains the following strains of virus:
attenuated Schwarz measles, RIT 4385 mumps derived from Jeryl Lynn strain and Wistar RA 27/3 rubella strains of viruses.
Priorix Vaccine Page
Though there have been differing strains of measles and rubella employed, this article is concerned with the mumps strains employed in the vaccines. According to a 1994 US government report on vaccine adverse events, there are three main strains of mumps used in MMR vaccinations: Jeryl Lynn, Leningrad-3-Parkow, and Urabe AM9. There have been differing vaccines using these strains, for example, both Priorix and MMR II use the Jeryl Lynn strain of mumps. There have also been multiple MMR vaccinations using the Urabe AM9 strain; the main two of concern in this article are Trivirix/Pluserix (two names for the same vaccine – the former used in Canada, the latter elsewhere) and Immravax. Although there is evidence that other strains of mumps virus used in MMR can cause aseptic meningitis as well, the Urabe strain has a significantly higher risk of this than the Jeryl Lynn strain based on the clinical data.
The Introduction of Urabe Strain MMR & Adverse Events
Although Canada used the MMR vaccine previously, the Urabe strain MMR was first introduced in Canada in 1986. In the UK, the MMR vaccine was introduced for the first time in 1988, and two out of the three vaccines that were used contained the Urabe strain mumps. Japan introduced these vaccines in 1989.
One significant side effect of these vaccinations was aseptic meningitis:
Aseptic meningitis refers to inflammation of the meninges [area surrounding brain and spinal cord], not of the brain. It can result from a variety of infectious, toxic, chemical, or physical agents. No bacterial organism can be identified in or isolated from the cerebrospinal fluid, but serologic studies often implicate a viral etiology.
Adverse Events following Childhood Vaccines
According to the CDC, the symptoms are as follows:
- Fever
- Headache
- Stiff neck
- Photophobia (eyes being more sensitive to light)
- Sleepiness or trouble waking up from sleep
- Nausea
- Irritability
- Vomiting
- Lack of appetite
- Lethargy (a lack of energy)
It is possible for long-term harm to result, however, many cases resolve without long-term sequelae.
This section will discuss the evidence in detail for the conclusion that specifically the Urabe strain mumps component in these MMR vaccines causes aseptic meningitis. I will discuss multiple case reports and studies on this topic from medical journals in order to demonstrate the large amount of evidence that this vaccine causes aseptic meningitis and I will discuss the different article in the medical literature, in age order, starting with the earliest first. I will look at full articles when available and also abstracts where full articles are paywalled.
An early case report from Canada (dating from 1986, published in the medical literature 1988) reports a 14-year-old girl developing aseptic meningitis from a Urabe strain vaccine:
In October 1986 a 14-year-old girl with no history of measles-mumps-rubella vaccination was given Trivirix vaccine […] 26 days later […] she had clinical signs of aseptic meningitis.
A case of mumps meningitis: a complication of vaccination?
Another Canadian source, an article published in the Pediatric Infectious Disease Journal in 1989, has the following to say:
All cases of mumps meningoencephalitis diagnosed at our institution during the past 15 years were reviewed. There were […] 5 [cases] in 1986 to 1988. Four of the recent cases occurred 19 to 26 days after receipt of a new mumps vaccine (Urabe Am 9 strain) released in Canada in 1986.
Clinical and epidemiologic features of mumps meningoencephalitis and possible vaccine-related disease
There is no other information provided in the abstract about the course of illness in the 4 cases. The US 1994 government document mentioned above discussing the study states than none of the 4 children had sequelae in this study.
An article from the British Medical Journal, 1989, discusses another proven case of aseptic meningitis after Pluserix:
[W]e also hesitated before reporting a girl aged 3 years and 2 months who developed proved mumps meningitis 21 days after being given mumps, measles, and rubella immunisation (Pluserix). […] The mumps virus isolated from her cerebrospinal fluid was identical with the Urabe vaccine strain used in her immunisation.
Mumps meningitis after mumps, measles, and rubella vaccination
Another case report from the British context was published in the Lancet:
In 1989, Gray and Burns published two letters (Gray and Burns, 1989a,b) in The Lancet concerning a 3-year-old girl presenting with aseptic meningitis 21 days after vaccination with MMR. Fluorescent-antibody tests identified the isolated virus as mumps virus (Gray and Burns, 1989a), and soon thereafter, this virus was identified by nucleotide sequencing analysis as the Urabe strain (Gray and Burns, 1989b).
Adverse Events Associated with Childhood Vaccines: Evidence Bearing on Causality.
A 1991 article discusses Japan, where the Urabe vaccine was introduced in 1989. Japan had exactly the same issues with this vaccination as the UK and Canada:
Thirty-five children developed meningitis within 2 months after MMR vaccination during the 8-month period extending from April to November, 1989. The time lag between MMR vaccination and meningitis ranged from 14 to 28 days in the 35 cases of meningitis. The incidence of aseptic meningitis with positive mumps vaccine virus was estimated to be 0.11% (0.3% as a whole) during the 8 months from April to November and increased to 0.3% (0.7% as a whole) in September and October. We conclude that the incidence of aseptic meningitis after MMR vaccination seems to be higher than that reported previously.
A prefecture-wide survey of mumps meningitis associated with measles, mumps and rubella vaccine
Another article looking at Japan, again from 1991:
Among 630,157 recipients of measles-mumps-rubella trivalent (MMR) vaccine containing the Urabe Am9 mumps vaccine, there were at least 311 meningitis cases suspected to be vaccine-related. Meningitis was generally mild and there were no sequelae from the illness. The complication was more frequent among male than among female children.
Aseptic meningitis as a complication of mumps vaccination
For reference, the rate of Urabe strain mumps MMR vaccine meningitis would work out at about 1 in 2000 from this study.
A 1993 letter to the editor of the Archives of Disease in Childhood discusses underreporting of this vaccine complication:
Vaccine associated mumps meningitis was one of the conditions reportable to the British Paediatric Surveillance Unit (BPSU) between February 1990 and January 1992. During this two year period, 15 confirmed cases were reported. […] Based on the BPSU study the estimated risk of vaccine associated mumps meningitis in this age group was 1.5 per 100 000 vaccinations given. However when the BPSU data were supplemented by laboratory reports, a much higher rate of approximately 10 per 100 000 vaccinations was observed.
Reporting of vaccine associated mumps meningitis
A 1996 article, this time from France, sought to retroactively assess the risk of this vaccination:
Fifty-four cases of AM were reported to the regional drug surveillance centres or to the manufacturer from the time each vaccine was launched up until June 1992. Twenty cases were associated with the time off administration of a monovalent mumps vaccine and 34 with a trivalent measles, mumps and rubella vaccine (MMR).[…] The global incidence of mumps vaccine-associated AM was 0.82/100,000 doses, which is significantly lower than the incidence in the unvaccinated population.
Aseptic meningitis after mumps vaccination
A 1996 study from Japan sought to compare the risks of Urabe containing MMR vaccines with other MMR vaccines.
The rates of virologically confirmed aseptic meningitis per 10 000 recipients were 16.6 for the standard MMR [i.e. containing Urabe strain mumps]
Adverse events associated with MMR vaccines in Japan
The rate was lower for the other MMR vaccinations.
A 1999 article acknowledges:
Aseptic meningitis is a well documented adverse event (1-4) that is attributable to the Urabe mumps strain of the combined measles-mumps-rubella (MMR) vaccine.
Outbreak of aseptic meningitis associated with mass vaccination with a urabe-containing measles-mumps-rubella vaccine: implications for immunization programs
There was a mass vaccination campaign in Salvador, Brazil with the Urabe strain MMR vaccine Pluserix. The vaccination campaign en masse injected children from 1-11 within a very short period of time, just a couple of weeks. There was a significant spike in aseptic meningitis 3 weeks after ‘Vaccination Day’, providing further evidence of the dangers of this vaccine:
We conservatively estimated the risk of aseptic meningitis to be 1 in 14,000 doses (32 cases out of 452,344 applied doses).
A 2007 article attempts to assess the risk of aseptic meningitis with the Jeryl Lynn strain vis-a-vis the Urabe strain. It states that of 6 cases identified in computerised records between Jan 1991-Sep 1992, 4 were most likely triggered by a Urabe strain MMR vaccine. It further observes that the rate of aseptic meningitis from these vaccines can be estimated at about 1/12,500, and that:
The real risk of acute neurologic consequences from the Urabe mumps component of MMR was underestimated when using case ascertainment methods that were reliant on laboratory investigations
Risks of Convulsion and Aseptic Meningitis following Measles-Mumps-Rubella Vaccination in the United Kingdom
As we can see from the above evidence, there are a multitude of different estimates of the rate of Urabe strain-induced vaccine meningitis. The Japanese articles give the highest estimates, with 16.6/10,000 [1 in ~602] and 311/630,157 [1 in ~2000]. Surveillance was more intense in the Japanese context, with the 1996 study that gives us 16.6/10000 being based on active surveillance. This means the study authors are actively looking for the adverse event, rather than passive surveillance where something only gets flagged up when it happens to be reported by a doctor or patient (such as VAERS or Yellow Card). This will lead to a higher number of cases reported.
Other articles originating in other countries give a lower estimate of aseptic meningitis. These articles seem to be based on retroactive studies of hospital admissions for aseptic meningitis and may be less complete than studies based upon active surveillance. Nevertheless they still give a rate of around 1 in 14,000-1 in 10,000.
However all these articles are agreed in either the suspicion or the fact that the Urabe strain MMR does cause aseptic meningitis. In many cases discussed the Urabe strain mumps was found in patient samples. In other words there is no real debate about this: the vaccine causes aseptic meningitis. I could not find a single article dissenting from the view that the vaccine is responsible for at least some observed cases of aseptic meningitis.
Political and Medical Corruption Behind the Urabe MMR Vaccine
We are immunising the children and the government is immunising us.
SmithKline Representative to MMR whistleblower, as reported to Andrew Wakefield (Callous Disregard, p. 68)
This section will focus on the UK situation only, and not upon the introduction and use of this vaccine in other countries.
Let’s start with the Guidelines for the MMR vaccination, published in the British Medical Journal in 1988 [the vaccine was introduced in October of that year]:
The vaccine will be available from two manufacturers, Smith Kline and French [Trivirix/Pluserix] and Merieux UK [Immravax]; both vaccines contain the same strains of virus: Mumps; Urabe AMI9. This has been in use in the Smith Kline and French vaccine in Europe and Asia for three to four years.
Measles, mumps, and rubella vaccine: The following guidelines on the use of the measles, mumps, and rubella vaccine have been sent by the Department of Health to all general practitioners.
The comment relating to the Urabe strain is clearly meant to imply that it is safe for use, since if if has been in use for 3-4 years, that makes it safe, right? Interestingly, there is no comment in this document regarding the strain of measles or rubella, indicating a defensiveness about the mumps vaccine strain in use.
The ‘Adverse reactions’ section says the following (in full):
As with measles vaccine, malaise, fever and/or a rash may occur, most commonly about a week after vaccination and lasting about two to three days. Parotid swelling [glands near the jaw] occasionally occurs, usually in the third week; children with postvaccination symptoms are not infectious. Parents will be given information and advice for reducing fever, including the use of paracetamol in the period 5-10 days after vaccination. Serious reactions should be reported to the Committee on Safety of Medicines using the yellow card system.
As we can see, there is no reference to the possibility of aseptic meningitis in this section. However, as we can see from the above literature, the possibility of aseptic meningitis had already been raised as an issue in the Canadian context, with cases of aseptic meningitis having been reported very soon after the vaccine’s introduction, with the two articles above from Canada highlighting some of these cases.
However it gets worse. Not only were there cases in Canada, but:
Pluserix had been licensed in numerous countries prior to 1988 but unbeknown to the British public, far from it having a good record in these countries, the vaccine had already been withdrawn in Canada, where it had been marketed as Trivirix, following the discovery of adverse reactions of aseptic meningitis. [original emphasis]
The Urabe Farrago
The Canadian Chief Medical Officer of the Ontario Ministry of Health stated all of these vaccines had to be sent back and no longer used in July 1988. Canada eventually went further and pulled the license of the vaccine in 1990.
The UK decided, essentially, to ignore the Canadian experience with these vaccines and introduce them anyway in 1988. When assessing the safety of the MMR vaccine, they used irrelevant data from countries using a completely different MMR vaccination, such as the US. This data was accepted as relevant despite the differences in the vaccinations. They rushed through a license for the Pluserix vaccine, in order that their announced MMR program could go forward as per schedule. Furthermore, the whistleblower mentioned at the top of this section, who had worked in the Canadian system and seen the harms of the vaccine, advised the JCVI that it should not be used, but he was ignored by more senior members.
As mentioned in the header, it appears the company SmithKline had no liability for these vaccinations and adverse events caused by them. Instead the government seemed to be the party liable. This situation continued; the JCVI minutes in 1993 state that the manufacturers “continue to sell the Urabe MMR without liability” (cited in Callous Disregard, p. 74). The UK stopped using the vaccines in 1992, but did not pull the license which helped to enable the use of the vaccine in other countries (such as Brazil in 1997 – see above cited article). This meant injuries caused by these vaccines continued to occur.
What can we conclude? The main concern of the UK authorities was not to ensure the safety of the vaccine, but to ensure the political success of the MMR program.
There are very powerful people in positions of great authority who have staked their reputations on the safety of MMR and they are willing to do almost anything to protect themselves.
Dr. Peter Fletcher
Conclusion
The success of a vaccination program, as defined by the establishment, has nothing to do with the safety or effectiveness of a vaccine. Instead, it is purely a political and religious construct about getting needles in arms. The corruption in vaccination programs is not a new development with the ‘Covid-19 pandemic’, instead it has existed in previous vaccine campaigns.
Appendix: Personal Comments on Urabe Strain Mumps MMR.
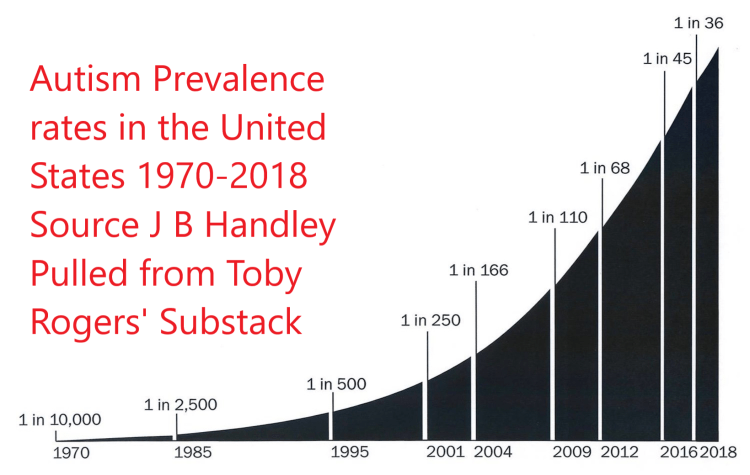
I received the MMR vaccine in 1989. At the time, 85-90% (different sources give slightly different figures) of the MMR vaccinations in use in the UK contained the Urabe strain mumps. As aseptic meningitis is a specific form of inflammation around the brain, it is not far fetched to suggest a possible link to autism (given that autism is an inflammatory disease) – although as far as I’m aware there has been no direct evidence regarding this question. Of course, the US, with its skyrocketing rates of autism never used these specific vaccines, and MMR vaccination is not the only factor to consider in autism.
With this in mind, I tried to find out specifically which MMR vaccination I received, so I wrote to my GP surgery and asked for the ‘brand and/or batch/lot’ of MMR vaccine I received. They sent me my vaccination records, which appears to not contain this information, so I was not able to confirm whether I received a Urabe-containing vaccine. However, I did receive a message from the GP surgery on my letter enclosed with the vaccination records that the surgery is a “Vaccine Positive practice” that “Vaccination is one of the greatest success stories in modern medicine” and that it “saves lives and prevents suffering.” Bear in mind, the only question I asked was about the brand and batch/lot of MMR vaccine I received: I made no reference to adverse events in any way. Apparently even asking about this basic information is too much of a question for the vaccination cult.
Image Via Openverse.